Potrebbero piacerti anche
- My Personal and Final Wishes: Things You Need to KnowDa EverandMy Personal and Final Wishes: Things You Need to KnowNessuna valutazione finora
- Application FormDocumento2 pagineApplication FormAzhar AbbasNessuna valutazione finora
- One PieceDocumento2 pagineOne Piecearisht.pokharnaNessuna valutazione finora
- Student registration formDocumento2 pagineStudent registration formUday Kumar SinghNessuna valutazione finora
- Application Form TitleDocumento1 paginaApplication Form TitleEngrAneelKumarAkhaniNessuna valutazione finora
- Friends and Music: Member Data SheetDocumento1 paginaFriends and Music: Member Data SheetLorieCuevasNessuna valutazione finora
- Register to volunteer with SENSE abilityDocumento2 pagineRegister to volunteer with SENSE abilityAnonymous nzEABag5KVNessuna valutazione finora
- Ch. Pervaiz Elahi Institute of Cardiology, MultanDocumento1 paginaCh. Pervaiz Elahi Institute of Cardiology, MultanAdnan RasikhNessuna valutazione finora
- Bio Data FormDocumento8 pagineBio Data FormChrls AjrNessuna valutazione finora
- Application Form: Name of Office Post Beginning Date Ending DateDocumento1 paginaApplication Form: Name of Office Post Beginning Date Ending DateSaher SeherNessuna valutazione finora
- Bio-Data FormDocumento1 paginaBio-Data FormMark Jellicoe Pascual RodillasNessuna valutazione finora
- Bio Data Sheet 1Documento1 paginaBio Data Sheet 1VeeJay Del Rosario75% (130)
- Matrimony - Application FormDocumento1 paginaMatrimony - Application FormMarian ToquireNessuna valutazione finora
- Bio DataDocumento1 paginaBio Datamolina.bervettehansNessuna valutazione finora
- Membership ProfileDocumento1 paginaMembership Profileapi-250958742Nessuna valutazione finora
- Rental Application FormDocumento2 pagineRental Application Formobinna udenzeNessuna valutazione finora
- BIO Data (Lalu)Documento1 paginaBIO Data (Lalu)Herbert Quimada RebloraNessuna valutazione finora
- Women's Education Academy Admission FormDocumento2 pagineWomen's Education Academy Admission FormmzeqtaNessuna valutazione finora
- ApplicationDocumento2 pagineApplicationLokesh RaoNessuna valutazione finora
- CEDCOS Form Jan 24 PDFDocumento1 paginaCEDCOS Form Jan 24 PDFYaseen AkhtarNessuna valutazione finora
- Please Enclose A Photocopy of Your Picture ID For Certified CopiesDocumento1 paginaPlease Enclose A Photocopy of Your Picture ID For Certified CopiesJazzy KateNessuna valutazione finora
- Biodata Format For JobDocumento1 paginaBiodata Format For JobFairoza Fidelyn Villaruz50% (2)
- Scholarship FormDocumento1 paginaScholarship Formgraham5333Nessuna valutazione finora
- Ministry of Human Rights: Affix Passport Size PhotographDocumento1 paginaMinistry of Human Rights: Affix Passport Size PhotographMuhammad JunaidNessuna valutazione finora
- New Application Form For Recruitment 2020Documento1 paginaNew Application Form For Recruitment 2020امین ثانیNessuna valutazione finora
- Teacher's ProfileDocumento1 paginaTeacher's ProfileShim CharenNessuna valutazione finora
- Confirmation Registration FormDocumento1 paginaConfirmation Registration FormLucy SalasNessuna valutazione finora
- PDF Form - Talent Info Sheet 2016Documento1 paginaPDF Form - Talent Info Sheet 2016Jonathan EugenioNessuna valutazione finora
- Upload Your CV by Filling This Form: Personal InformationDocumento2 pagineUpload Your CV by Filling This Form: Personal Informationzeeshanshani1118Nessuna valutazione finora
- Membership-Form RF01Documento1 paginaMembership-Form RF01paulo jongNessuna valutazione finora
- Membership-Form RF01Documento1 paginaMembership-Form RF01G BoyNessuna valutazione finora
- Music Team Membership Form: United Pentecostal Church of The Philippines, IncDocumento2 pagineMusic Team Membership Form: United Pentecostal Church of The Philippines, IncJake AriñoNessuna valutazione finora
- Membership ApplicationDocumento1 paginaMembership Applicationjennie_malteseNessuna valutazione finora
- Bio Data FormDocumento1 paginaBio Data FormCecile Flores CorveraNessuna valutazione finora
- Art Ad. Registration Final WordDocumento2 pagineArt Ad. Registration Final WordEmmaChalifourNessuna valutazione finora
- Bi O-Dat Aco Pyri Ghted-140725050745-Phpapp01Documento2 pagineBi O-Dat Aco Pyri Ghted-140725050745-Phpapp01philip resuello100% (1)
- Report of Birth FormDocumento1 paginaReport of Birth FormFelomina Glee Ayupan PalmaNessuna valutazione finora
- New Enrolment Application Form 2013 1Documento1 paginaNew Enrolment Application Form 2013 1api-249113075Nessuna valutazione finora
- Personal data form BONGADocumento2 paginePersonal data form BONGAemanNessuna valutazione finora
- Personal Data Sheet TemplateDocumento1 paginaPersonal Data Sheet TemplateLenrick BancilNessuna valutazione finora
- Candidate Introduction Form: Please Affix Your Photograph HereDocumento1 paginaCandidate Introduction Form: Please Affix Your Photograph HeremadhursibalNessuna valutazione finora
- Registration FormDocumento1 paginaRegistration FormVanessaTanNessuna valutazione finora
- Job Application Form TitleDocumento2 pagineJob Application Form TitleOwais ZamanNessuna valutazione finora
- NameDocumento1 paginaNameapi-137263928Nessuna valutazione finora
- Date of Marriage: - Time: - PlaceDocumento2 pagineDate of Marriage: - Time: - PlaceRosanna RebueltoNessuna valutazione finora
- Mohi-Ud-Din Islamic University: Academic Data/ Professional QualificationsDocumento1 paginaMohi-Ud-Din Islamic University: Academic Data/ Professional QualificationsAhmad JunaidNessuna valutazione finora
- Barangay Information SheetDocumento6 pagineBarangay Information SheetSagud Bahley Brgy CouncilNessuna valutazione finora
- resume-3Documento1 paginaresume-3samueldomalaon1970Nessuna valutazione finora
- Christian Life Program Information Sheet for CouplesDocumento1 paginaChristian Life Program Information Sheet for Coupleseslima5100% (1)
- First Holy Communion Registration FormDocumento1 paginaFirst Holy Communion Registration FormLucy SalasNessuna valutazione finora
- Homework Club: Children Must Be 9 Years and Older To AttendDocumento2 pagineHomework Club: Children Must Be 9 Years and Older To AttendEmmaChalifourNessuna valutazione finora
- Formulir Isian UsaDocumento5 pagineFormulir Isian UsaFika FebrianaNessuna valutazione finora
- Apply Online - Job Application FormDocumento1 paginaApply Online - Job Application Formzamanrana92Nessuna valutazione finora
- Jowa Application Form 2Documento2 pagineJowa Application Form 2Kaye AnneNessuna valutazione finora
- Application Form: Personal InformationDocumento2 pagineApplication Form: Personal InformationMuzamil HussainNessuna valutazione finora
- Program Applying For:: Application FormDocumento3 pagineProgram Applying For:: Application FormChesya BwanausiNessuna valutazione finora
- Free Printable Rental ApplicationDocumento2 pagineFree Printable Rental ApplicationHolly Chalmers HillerNessuna valutazione finora
- HR Director Job Application FormDocumento3 pagineHR Director Job Application FormKashif RaheemNessuna valutazione finora
- Registration FormDocumento2 pagineRegistration FormJoseph MontellsNessuna valutazione finora
- Personal Data: Middle Name First Name Last NameDocumento1 paginaPersonal Data: Middle Name First Name Last NameKim Joshua SaoitNessuna valutazione finora
- Project analysis of an aluminum structureDocumento9 pagineProject analysis of an aluminum structureMuhammad UmairNessuna valutazione finora
- CV - (Muhammad Umair) PDFDocumento1 paginaCV - (Muhammad Umair) PDFMuhammad UmairNessuna valutazione finora
- Vat With FlangDocumento1 paginaVat With FlangMuhammad UmairNessuna valutazione finora
- ReferencesDocumento1 paginaReferencesMuhammad UmairNessuna valutazione finora
- Chlorine Dioxide Material CompatibilityDocumento3 pagineChlorine Dioxide Material CompatibilityMuhammad UmairNessuna valutazione finora
- Neelum Jhelum Hydropower Project: Internship ReportDocumento1 paginaNeelum Jhelum Hydropower Project: Internship ReportMuhammad UmairNessuna valutazione finora
- Part Number SDAF 22330, Inch Straight Bore Mounting Pillow Block SDAF222 and SDAF223 SeriesDocumento3 paginePart Number SDAF 22330, Inch Straight Bore Mounting Pillow Block SDAF222 and SDAF223 SeriesMuhammad UmairNessuna valutazione finora
- Equivalent Stress Calculation ReportDocumento1 paginaEquivalent Stress Calculation ReportMuhammad UmairNessuna valutazione finora
- Strain EnergyDocumento1 paginaStrain EnergyMuhammad UmairNessuna valutazione finora
- Objective: Design Specifications:: Problem StatementDocumento2 pagineObjective: Design Specifications:: Problem StatementMuhammad UmairNessuna valutazione finora
- Yu-Jing He, Ya-Dong Tang, Jing-Zhao Shi and He Li: Finite Element Analysis of The Loader Boom Based On ABAQUSDocumento6 pagineYu-Jing He, Ya-Dong Tang, Jing-Zhao Shi and He Li: Finite Element Analysis of The Loader Boom Based On ABAQUSMuhammad UmairNessuna valutazione finora
- F Chapter4Documento14 pagineF Chapter4Muhammad UmairNessuna valutazione finora
- Operation Manual Safety Principles, Operation and MaintenanceDocumento12 pagineOperation Manual Safety Principles, Operation and MaintenanceMuhammad UmairNessuna valutazione finora
- Spindelhubtisch-Spindel Lifting Table TASK PDFDocumento17 pagineSpindelhubtisch-Spindel Lifting Table TASK PDFMuhammad UmairNessuna valutazione finora
- Telecommunication EngineeringDocumento21 pagineTelecommunication EngineeringFarhanAhmedNessuna valutazione finora
- Signal System ObjectiveDocumento82 pagineSignal System ObjectiveNitin Kathuria100% (3)
- KemiraDocumento4 pagineKemiraMuhammad UmairNessuna valutazione finora
- The Solar ChimneyDocumento16 pagineThe Solar ChimneyMuhammad UmairNessuna valutazione finora
- Paper Manufacturers in PakistanDocumento7 paginePaper Manufacturers in PakistanMuhammad UmairNessuna valutazione finora
- FFC TestDocumento3 pagineFFC TestShehzad ChaudhryNessuna valutazione finora
- Valve SelectionDocumento8 pagineValve SelectionShreya Sahajpal KaushalNessuna valutazione finora
- Rachna College of Engineering & Technology, GujranwalaDocumento2 pagineRachna College of Engineering & Technology, GujranwalaMuhammad UmairNessuna valutazione finora
- TA436 03 BAL Piston Diaphragm Pump C409 2 KM enDocumento70 pagineTA436 03 BAL Piston Diaphragm Pump C409 2 KM enMuhammad UmairNessuna valutazione finora
- Paper Manufacturers in PakistanDocumento7 paginePaper Manufacturers in PakistanMuhammad UmairNessuna valutazione finora
- Boiler FORM NEW Photocopy Accepted PDFDocumento4 pagineBoiler FORM NEW Photocopy Accepted PDFSUKhan87% (15)
- Challan Form-21-05-2014 PDFDocumento1 paginaChallan Form-21-05-2014 PDFAila DarNessuna valutazione finora
- Cooling Tower Water Treatment ChemistryDocumento4 pagineCooling Tower Water Treatment ChemistryMuhammad UmairNessuna valutazione finora
- Brenntag Contract - Muhammad UmairDocumento10 pagineBrenntag Contract - Muhammad UmairMuhammad UmairNessuna valutazione finora
- Kemira Introductory ReportDocumento5 pagineKemira Introductory ReportMuhammad UmairNessuna valutazione finora
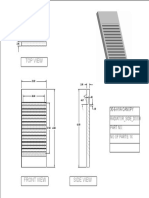
- Radiator Side Door Dimensions and ViewsDocumento1 paginaRadiator Side Door Dimensions and ViewsMuhammad UmairNessuna valutazione finora