Potrebbero piacerti anche
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (121)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (588)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (400)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (266)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5794)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (345)
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (895)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- List of Cranial NervesDocumento2 pagineList of Cranial NervesEunice A. EdaniolNessuna valutazione finora
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- Impact of Crossfit Related Spinal InjuriesDocumento4 pagineImpact of Crossfit Related Spinal Injuriesjoao manoelNessuna valutazione finora
- The Decompressive CraniectomyDocumento32 pagineThe Decompressive CraniectomyAmerican English CourseNessuna valutazione finora
- Cerebellar SyndromesDocumento10 pagineCerebellar SyndromesEmi Valcov100% (1)
- Textbook of Neural Repair and Rehabilitation Medical Neurorehabilitation 2006Documento802 pagineTextbook of Neural Repair and Rehabilitation Medical Neurorehabilitation 2006enigelNessuna valutazione finora
- 2015-01-01 Norms For The Health Cadre - Sri LankaDocumento83 pagine2015-01-01 Norms For The Health Cadre - Sri LankaDoctors News86% (7)
- Pathology of CNS TumorsDocumento58 paginePathology of CNS TumorsNaglaa RamadanNessuna valutazione finora
- Topics For Reporting in NCM 116Documento1 paginaTopics For Reporting in NCM 116Sarmiento, Jovenal B.Nessuna valutazione finora
- Nanos 2017Documento552 pagineNanos 2017Dalia MeiraNessuna valutazione finora
- Misdiagnosis of Gastroesophageal Reux Disease As Epileptic Seizures in ChildrenDocumento4 pagineMisdiagnosis of Gastroesophageal Reux Disease As Epileptic Seizures in ChildrenIoana IaruNessuna valutazione finora
- BrownGreer Response To Tighe 3/11/19Documento28 pagineBrownGreer Response To Tighe 3/11/19DeadspinNessuna valutazione finora
- Lecture Note Asas Psikologi (The Biological Perspective)Documento66 pagineLecture Note Asas Psikologi (The Biological Perspective)Muhammad FaizNessuna valutazione finora
- CSF Shift Edema PublishedDocumento15 pagineCSF Shift Edema PublishedIype CherianNessuna valutazione finora
- Critical Illness Polyneuropathy and Critical Illness Myopathy PDFDocumento5 pagineCritical Illness Polyneuropathy and Critical Illness Myopathy PDFAhraxazel Galicia ReynaNessuna valutazione finora
- AQ4PDocumento3 pagineAQ4PAhmed GaberNessuna valutazione finora
- Neurological Examination Made Practical PDFDocumento206 pagineNeurological Examination Made Practical PDFNorman VallejoNessuna valutazione finora
- AbipaDocumento3 pagineAbiparichy2hotNessuna valutazione finora
- Duchenne Muscular DystrophyDocumento18 pagineDuchenne Muscular DystrophyGnaa Puspita Sari PangeranNessuna valutazione finora
- Kapil Sethi - Paroxysmal Dyskinesias Newest-NO VIDEOSDocumento43 pagineKapil Sethi - Paroxysmal Dyskinesias Newest-NO VIDEOSMinerva StanciuNessuna valutazione finora
- Out PDFDocumento12 pagineOut PDFMaria RenjaanNessuna valutazione finora
- PTH Migraine LoopDocumento15 paginePTH Migraine LoopRenju KuriakoseNessuna valutazione finora
- The Best Evidence For Progressive Myoclonic Epilepsy - A Pathway To Precision TherapyDocumento11 pagineThe Best Evidence For Progressive Myoclonic Epilepsy - A Pathway To Precision TherapyHabib G. Moutran BarrosoNessuna valutazione finora
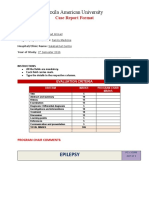
- Texila American University: Case Report FormatDocumento7 pagineTexila American University: Case Report FormatShahzad AhmadNessuna valutazione finora
- CSF (Cerebrospinal Fluid)Documento4 pagineCSF (Cerebrospinal Fluid)few10Nessuna valutazione finora
- IFS Validación ChilenaDocumento8 pagineIFS Validación Chilenapablo antonio roa espinozaNessuna valutazione finora
- Hearing Handicap Inventory For The Elderly (HHIE)Documento5 pagineHearing Handicap Inventory For The Elderly (HHIE)Is GutiérrezNessuna valutazione finora
- Multiple Choice Question Acn FinalDocumento11 pagineMultiple Choice Question Acn FinalIqra rizwanNessuna valutazione finora
- Project Report On Gait AnalysisDocumento16 pagineProject Report On Gait Analysisprikshitthakur7.comNessuna valutazione finora
- Meningioma: A Review of Epidemiology, Pathology, Diagnosis, Treatment, and Future DirectionsDocumento15 pagineMeningioma: A Review of Epidemiology, Pathology, Diagnosis, Treatment, and Future Directionswibawa suryaNessuna valutazione finora
- Types of Cerebral PalsyDocumento6 pagineTypes of Cerebral PalsySahil SahniNessuna valutazione finora