Potrebbero piacerti anche
- Best Practices For Elderly Hip Fracture Patients. A Systematic Overview of The Evidence.Documento7 pagineBest Practices For Elderly Hip Fracture Patients. A Systematic Overview of The Evidence.Tuấn Lê (jose)Nessuna valutazione finora
- 2015 - Article - 665eficacia EpicondilitiDocumento13 pagine2015 - Article - 665eficacia EpicondilitimorbreirNessuna valutazione finora
- Clinical Outcomes of Rehabilitation For Patients Following Lateral Patellar Dislocation: A Systematic ReviewDocumento13 pagineClinical Outcomes of Rehabilitation For Patients Following Lateral Patellar Dislocation: A Systematic ReviewHarshoi KrishannaNessuna valutazione finora
- Occupational Therapy For Rheumatoid Arthritis: A Systematic ReviewDocumento14 pagineOccupational Therapy For Rheumatoid Arthritis: A Systematic ReviewispasNessuna valutazione finora
- Stability of Treatment For Anterior Open-Bite Malocclusion: A Meta-AnalysisDocumento16 pagineStability of Treatment For Anterior Open-Bite Malocclusion: A Meta-AnalysisAndré DrumondNessuna valutazione finora
- Early MobilizationDocumento9 pagineEarly MobilizationBlake BoggenpoelNessuna valutazione finora
- LST 2016-08-04 Gsse Reading List 2017 PDFDocumento3 pagineLST 2016-08-04 Gsse Reading List 2017 PDFRGNessuna valutazione finora
- 2017 Article 528Documento12 pagine2017 Article 528Marios GhobrialNessuna valutazione finora
- File Jurnal VertigoDocumento12 pagineFile Jurnal VertigoChris JohnNessuna valutazione finora
- Manual Therapy: Susan Armijo-Olivo, Sharon Warren, Jorge Fuentes, David J. MageeDocumento10 pagineManual Therapy: Susan Armijo-Olivo, Sharon Warren, Jorge Fuentes, David J. MageeJu ChangNessuna valutazione finora
- HHS Public Access: Achalasia Treatment, Outcomes, Utilization, and Costs: A Population-Based Study From The United StatesDocumento12 pagineHHS Public Access: Achalasia Treatment, Outcomes, Utilization, and Costs: A Population-Based Study From The United StatesInomy ClaudiaNessuna valutazione finora
- CPHeadacheDocumento30 pagineCPHeadachedoctor_bunnyNessuna valutazione finora
- Current Databases On Biological Variation: Pros, Cons and ProgressDocumento10 pagineCurrent Databases On Biological Variation: Pros, Cons and ProgressCarlos PardoNessuna valutazione finora
- Journal ESWT Pada DewasaDocumento7 pagineJournal ESWT Pada DewasaPhilipusHendryHartonoNessuna valutazione finora
- Angle 2007 Vol. 77, No. 2, Pp. 376-381Documento6 pagineAngle 2007 Vol. 77, No. 2, Pp. 376-381André MéndezNessuna valutazione finora
- Academic Emergency Medicine - 2011 - RossDocumento9 pagineAcademic Emergency Medicine - 2011 - RossgomcoiteNessuna valutazione finora
- CRA 2010-Poster-PresentationsDocumento236 pagineCRA 2010-Poster-PresentationsJoe GassNessuna valutazione finora
- Manual TheraManual Therapy For Osteoarthritis of The Hip or KneepDocumento9 pagineManual TheraManual Therapy For Osteoarthritis of The Hip or KneepBwizerNessuna valutazione finora
- Jurnal Tendon 1Documento10 pagineJurnal Tendon 1hendrabecaxNessuna valutazione finora
- Original Research: Intensive Care Unit Structure Variation and Implications For Early Mobilization PracticesDocumento12 pagineOriginal Research: Intensive Care Unit Structure Variation and Implications For Early Mobilization Practicesandi kurniawanNessuna valutazione finora
- TB Tratamiento TempranoDocumento9 pagineTB Tratamiento TempranoteretransproteNessuna valutazione finora
- BR J Sports Med-2008-Hegedus-80-92 PDFDocumento14 pagineBR J Sports Med-2008-Hegedus-80-92 PDFAnonymous Jx2UvBeteNessuna valutazione finora
- Dexamethasone For Antiemesis in Laparoscopic.27Documento8 pagineDexamethasone For Antiemesis in Laparoscopic.27Yogo WibowoNessuna valutazione finora
- Afh 174Documento8 pagineAfh 174Muamar Ray AmirullahNessuna valutazione finora
- Enteral Versus Parenteral Nutrition in Critically Ill Patients - An Updated Systematic Review and Meta-Analysis of Randomized Controlled TrialsDocumento14 pagineEnteral Versus Parenteral Nutrition in Critically Ill Patients - An Updated Systematic Review and Meta-Analysis of Randomized Controlled TrialsLea Bali Ulina SinurayaNessuna valutazione finora
- Auriculotherapy For Pain Management: A Systematic Review and Meta-Analysis of Randomized Controlled TrialsDocumento12 pagineAuriculotherapy For Pain Management: A Systematic Review and Meta-Analysis of Randomized Controlled TrialsSol Instituto TerapêuticoNessuna valutazione finora
- Understanding Patient Provider Conversations: What Are We Talking About?Documento1 paginaUnderstanding Patient Provider Conversations: What Are We Talking About?drartzNessuna valutazione finora
- StrobeDocumento6 pagineStrobeAanh EduardoNessuna valutazione finora
- Oxford CEBM 2011 The 2011 Oxford CEBM Levels of EvidenceDocumento12 pagineOxford CEBM 2011 The 2011 Oxford CEBM Levels of EvidenceDenny AdriansyahNessuna valutazione finora
- Eating DisordersDocumento12 pagineEating DisordersYanuar AnggaraNessuna valutazione finora
- Stadhouder 2008 SpineDocumento12 pagineStadhouder 2008 SpineVijay JephNessuna valutazione finora
- Patient Centred Variables With Univariateassociations With Unplanned ICU Admissiona Systematic ReviewDocumento9 paginePatient Centred Variables With Univariateassociations With Unplanned ICU Admissiona Systematic ReviewsarintiNessuna valutazione finora
- Bernadeth P. Solomon BSN Lll-A The Effectiveness of Motorised Lumbar Traction in The Management of LBP With Lumbo Sacral Nerve Root Involvement: A Feasibility Study Annette A Harte1Documento5 pagineBernadeth P. Solomon BSN Lll-A The Effectiveness of Motorised Lumbar Traction in The Management of LBP With Lumbo Sacral Nerve Root Involvement: A Feasibility Study Annette A Harte1roonnNessuna valutazione finora
- (Extubação 3) 2012 Nursing in Critical Care-LibreDocumento12 pagine(Extubação 3) 2012 Nursing in Critical Care-Librec_henriqueamaral84Nessuna valutazione finora
- Vascaccess 1996 Randolph CCMDocumento7 pagineVascaccess 1996 Randolph CCMFARHAN BADRUZ ZAMAN mhsD4TEM2020RNessuna valutazione finora
- The Role of Triage Nurse Ordering. Brian H. Rowe, 2011 PDFDocumento9 pagineThe Role of Triage Nurse Ordering. Brian H. Rowe, 2011 PDFCristobal Alejandro Falado SantanderNessuna valutazione finora
- Palliative and Supportive CareDocumento16 paginePalliative and Supportive CareJoão AcupunturistaNessuna valutazione finora
- Rcsann 2016 0048Documento6 pagineRcsann 2016 0048fabian arassiNessuna valutazione finora
- Sedation Guidelines, Protocols, and Algorithms In.13Documento8 pagineSedation Guidelines, Protocols, and Algorithms In.13Juan Pedro Alconada MaglianoNessuna valutazione finora
- Artigo LIVE Fukuda (Menisco Hohmann2018)Documento10 pagineArtigo LIVE Fukuda (Menisco Hohmann2018)gabynieto.031090Nessuna valutazione finora
- Screenshot 2024-02-20 at 23.03.52Documento6 pagineScreenshot 2024-02-20 at 23.03.52qory fitrahtulNessuna valutazione finora
- Tumor Size Predicts Outcome in Pediatric Thyroid CancerDocumento6 pagineTumor Size Predicts Outcome in Pediatric Thyroid Cancerakshata patilNessuna valutazione finora
- Abat 2016Documento8 pagineAbat 2016toaldoNessuna valutazione finora
- A Review of Pain Management Interventions in Bone Marrow BiopsyDocumento9 pagineA Review of Pain Management Interventions in Bone Marrow BiopsyFikriNessuna valutazione finora
- A Framework For The Definition and Interpretation of The Use - 2023 - EclinicalDocumento12 pagineA Framework For The Definition and Interpretation of The Use - 2023 - Eclinicalronaldquezada038Nessuna valutazione finora
- Criteriul Variaţie Biologice Tabel (Dorite)Documento18 pagineCriteriul Variaţie Biologice Tabel (Dorite)Jimboreanu György Paula100% (1)
- BR J Sports Med-2008-Hegedus-80-92Documento14 pagineBR J Sports Med-2008-Hegedus-80-92api-263772125Nessuna valutazione finora
- Ultrasound-Guided Subclavian Vein Catheterization. A Systematic Review and Meta-Analysis. Crit Care Med 2015Documento10 pagineUltrasound-Guided Subclavian Vein Catheterization. A Systematic Review and Meta-Analysis. Crit Care Med 2015angelama1783riosNessuna valutazione finora
- ESWT-reviewMagnussen 2009Documento11 pagineESWT-reviewMagnussen 2009scsheenNessuna valutazione finora
- Biostatistics1718 1 PDFDocumento30 pagineBiostatistics1718 1 PDFSamNessuna valutazione finora
- Ilovepdf MergedDocumento22 pagineIlovepdf Mergedshirly tatianaNessuna valutazione finora
- Critical AppraisalDocumento9 pagineCritical Appraisalapi-402918352Nessuna valutazione finora
- Noninducibility in Postinfarction VT As An End Point For VT Ablation and Its Effects On Outcomes A Meta AnalysisDocumento14 pagineNoninducibility in Postinfarction VT As An End Point For VT Ablation and Its Effects On Outcomes A Meta AnalysisadytyaNessuna valutazione finora
- Medical Imaging.: ArticleDocumento6 pagineMedical Imaging.: ArticleAli AhmedNessuna valutazione finora
- Physioooo Research SamplesDocumento5 paginePhysioooo Research Samplesmeggan3Nessuna valutazione finora
- The Analytic Hierarchy Process in Medical and Health Care Decision Making: A Literature ReviewDocumento14 pagineThe Analytic Hierarchy Process in Medical and Health Care Decision Making: A Literature ReviewMarinelle TumanguilNessuna valutazione finora
- 10 1016@j Jclinepi 2004 04 005Documento8 pagine10 1016@j Jclinepi 2004 04 005ari_julian94Nessuna valutazione finora
- Epilepsy Duration and Seizure Outcome in Epilepsy Surgery: A Systematic Review and Meta-AnalysisDocumento9 pagineEpilepsy Duration and Seizure Outcome in Epilepsy Surgery: A Systematic Review and Meta-Analysisbaba ababNessuna valutazione finora
- Corticosteroids in The Treatment of Vestibular Neuritis: A Systematic Review and Meta-AnalysisDocumento7 pagineCorticosteroids in The Treatment of Vestibular Neuritis: A Systematic Review and Meta-AnalysisshiloinNessuna valutazione finora
- Diagnostic Problems in Tumors of Central Nervous System: Selected TopicsDa EverandDiagnostic Problems in Tumors of Central Nervous System: Selected TopicsNessuna valutazione finora
- Unit 2 - Programming of 8085 MicroprocessorDocumento32 pagineUnit 2 - Programming of 8085 MicroprocessorSathiyarajNessuna valutazione finora
- Bajaj Allianz General Insurance Company LimitedDocumento9 pagineBajaj Allianz General Insurance Company LimitedNaresh ChanchadNessuna valutazione finora
- Álvaro García Linera A Marxist Seduced BookDocumento47 pagineÁlvaro García Linera A Marxist Seduced BookTomás TorresNessuna valutazione finora
- Principle of Utmost Good FaithDocumento7 paginePrinciple of Utmost Good FaithshreyaNessuna valutazione finora
- Sky Education: Organisation of Commerce and ManagementDocumento12 pagineSky Education: Organisation of Commerce and ManagementKiyaara RathoreNessuna valutazione finora
- Asia Competitiveness ForumDocumento2 pagineAsia Competitiveness ForumRahul MittalNessuna valutazione finora
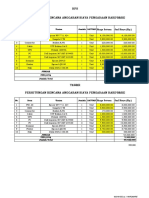
- HPS Perhitungan Rencana Anggaran Biaya Pengadaan Hardware: No. Item Uraian Jumlah SATUANDocumento2 pagineHPS Perhitungan Rencana Anggaran Biaya Pengadaan Hardware: No. Item Uraian Jumlah SATUANYanto AstriNessuna valutazione finora
- Invoice Inv0006: Er. Mohamed Irshadh P MDocumento1 paginaInvoice Inv0006: Er. Mohamed Irshadh P Mmanoj100% (1)
- Module 3 - Risk Based Inspection (RBI) Based On API and ASMEDocumento4 pagineModule 3 - Risk Based Inspection (RBI) Based On API and ASMEAgustin A.Nessuna valutazione finora
- Rainin Catalog 2014 ENDocumento92 pagineRainin Catalog 2014 ENliebersax8282Nessuna valutazione finora
- Timpuri Verbale Engleza RezumatDocumento5 pagineTimpuri Verbale Engleza RezumatBogdan StefanNessuna valutazione finora
- Total Product Marketing Procedures: A Case Study On "BSRM Xtreme 500W"Documento75 pagineTotal Product Marketing Procedures: A Case Study On "BSRM Xtreme 500W"Yasir Alam100% (1)
- NAME: - CLASS: - Describing Things Size Shape Colour Taste TextureDocumento1 paginaNAME: - CLASS: - Describing Things Size Shape Colour Taste TextureAnny GSNessuna valutazione finora
- Special Blood CollectionDocumento99 pagineSpecial Blood CollectionVenomNessuna valutazione finora
- Amadora V CA Case DigestDocumento3 pagineAmadora V CA Case DigestLatjing SolimanNessuna valutazione finora
- LESSON 2 - Nguyễn Thu Hồng - 1917710050Documento2 pagineLESSON 2 - Nguyễn Thu Hồng - 1917710050Thu Hồng NguyễnNessuna valutazione finora
- STD Symptoms, Causes and PreventionDocumento3 pagineSTD Symptoms, Causes and PreventionSakshi TyagiNessuna valutazione finora
- TAFC R10 SP54 Release NotesDocumento10 pagineTAFC R10 SP54 Release NotesBejace NyachhyonNessuna valutazione finora
- 4TH Quarter English 10 Assessment TestDocumento6 pagine4TH Quarter English 10 Assessment TestafbnjkcdNessuna valutazione finora
- Indian Wall Paintings - Analysis of Materials and TechniquesDocumento7 pagineIndian Wall Paintings - Analysis of Materials and Techniquesshu_sNessuna valutazione finora
- Httpswww.ceec.Edu.twfilesfile Pool10j07580923432342090202 97指考英文試卷 PDFDocumento8 pagineHttpswww.ceec.Edu.twfilesfile Pool10j07580923432342090202 97指考英文試卷 PDFAurora ZengNessuna valutazione finora
- Asian Paints SmartCare Damp Proof Warranty for TerracesDocumento11 pagineAsian Paints SmartCare Damp Proof Warranty for Terracesiman.krisman2109Nessuna valutazione finora
- Costco Case StudyDocumento3 pagineCostco Case StudyMaong LakiNessuna valutazione finora
- HLT42707 Certificate IV in Aromatherapy: Packaging RulesDocumento2 pagineHLT42707 Certificate IV in Aromatherapy: Packaging RulesNilamdeen Mohamed ZamilNessuna valutazione finora
- 1 Ancient-IndiaDocumento14 pagine1 Ancient-Indiakaushik joshiNessuna valutazione finora
- Marylebone Construction UpdateDocumento2 pagineMarylebone Construction UpdatePedro SousaNessuna valutazione finora
- Annexure 2 Form 72 (Scope) Annexure IDocumento4 pagineAnnexure 2 Form 72 (Scope) Annexure IVaghasiyaBipinNessuna valutazione finora
- Soap - WikipediaDocumento57 pagineSoap - Wikipediayash BansalNessuna valutazione finora
- Soil Mechanics: Principle of Effective Stress, Capillarity and Permeability On SoilDocumento54 pagineSoil Mechanics: Principle of Effective Stress, Capillarity and Permeability On SoilAwadhiNessuna valutazione finora
- Miriam Garcia Resume 2 1Documento2 pagineMiriam Garcia Resume 2 1api-548501562Nessuna valutazione finora