Potrebbero piacerti anche
- Introduction to Petroleum Process SafetyDa EverandIntroduction to Petroleum Process SafetyValutazione: 3 su 5 stelle3/5 (2)
- Quality Control OF Bulk Drug FormulationsDa EverandQuality Control OF Bulk Drug FormulationsNessuna valutazione finora
- Runaway Chemical Reaction and Vapor Cloud Explosion at Synthron FacilityDocumento17 pagineRunaway Chemical Reaction and Vapor Cloud Explosion at Synthron FacilityThing90Nessuna valutazione finora
- Bangot - CaseStudy01 - Synthron Explosion PDFDocumento5 pagineBangot - CaseStudy01 - Synthron Explosion PDFCj BangotNessuna valutazione finora
- Explosion X Reaccion Descontr de Polimero Acrilico FGyS - 9 Ago 07 PDFDocumento17 pagineExplosion X Reaccion Descontr de Polimero Acrilico FGyS - 9 Ago 07 PDFjuan_balderramaNessuna valutazione finora
- ReportDocumento25 pagineReportMohd Hafiz AhmadNessuna valutazione finora
- Case StudyDocumento13 pagineCase StudyYustinus Selis ToronNessuna valutazione finora
- SEPT 2022 - CLD 20002 - Chap 1 - Industrial SafetyDocumento104 pagineSEPT 2022 - CLD 20002 - Chap 1 - Industrial SafetyAirish AirishNessuna valutazione finora
- Case Studymajor Chemical Disasters FILEminimizerDocumento73 pagineCase Studymajor Chemical Disasters FILEminimizeridigitiNessuna valutazione finora
- Formosa Plastics Fire Case Study: Evaluating Process HazardsDocumento16 pagineFormosa Plastics Fire Case Study: Evaluating Process HazardsSaurabh ShahNessuna valutazione finora
- Safety Alert - Fire and Explosion Risk - Reactive MonomersDocumento2 pagineSafety Alert - Fire and Explosion Risk - Reactive MonomersSteve ForsterNessuna valutazione finora
- Case Study Major Chemical Disasters File MinimizeDocumento73 pagineCase Study Major Chemical Disasters File MinimizeAyush ShrimalNessuna valutazione finora
- Safety and Major Chemical DisastersDocumento30 pagineSafety and Major Chemical DisastersganeshNessuna valutazione finora
- Case Study On Major Chemical DisastersDocumento6 pagineCase Study On Major Chemical DisastersMukund P RaoNessuna valutazione finora
- 1 - Introduction To Chemical Process IndustriesDocumento13 pagine1 - Introduction To Chemical Process IndustriesVenus Abigail GutierrezNessuna valutazione finora
- Goodyear Houston Ammonia Release Case StudyDocumento10 pagineGoodyear Houston Ammonia Release Case StudyMas Arman TewoNessuna valutazione finora
- Basic Principle in CPIDocumento28 pagineBasic Principle in CPIDion VixNessuna valutazione finora
- Chemical Reaction Safety: Paul Sharratt 19 August 2019Documento32 pagineChemical Reaction Safety: Paul Sharratt 19 August 2019Chuah Chong YangNessuna valutazione finora
- Epcsm Term PaperDocumento13 pagineEpcsm Term PaperFake accNessuna valutazione finora
- CH3044 Plant Safety and Loss PreventionDocumento4 pagineCH3044 Plant Safety and Loss PreventionAchini NawarathnaNessuna valutazione finora
- Osha Individual ReportDocumento9 pagineOsha Individual ReportpuraniNessuna valutazione finora
- CompilationDocumento7 pagineCompilationQistyNessuna valutazione finora
- Why Use Silicones in Personal Care Part 1Documento8 pagineWhy Use Silicones in Personal Care Part 1JulioNessuna valutazione finora
- Assignment 3-Case Study PDFDocumento7 pagineAssignment 3-Case Study PDFazhani rosliNessuna valutazione finora
- G.chem Bhopal Gas TragedyDocumento16 pagineG.chem Bhopal Gas Tragedymrmy88tm46Nessuna valutazione finora
- Reactive Polymer ProcessingDocumento12 pagineReactive Polymer ProcessingVanNessuna valutazione finora
- Propylene ProductionDocumento1 paginaPropylene ProductionWade ColemanNessuna valutazione finora
- Machinery Safety Xbos 3103Documento11 pagineMachinery Safety Xbos 3103abdulhafidzrc939Nessuna valutazione finora
- The Bhopal Gas Tragedy: A Case Study on the World's Worst Industrial DisasterDocumento41 pagineThe Bhopal Gas Tragedy: A Case Study on the World's Worst Industrial DisasterVivek GurjarNessuna valutazione finora
- HIRA-Assignment 2Documento4 pagineHIRA-Assignment 2Naveen PrakashNessuna valutazione finora
- An Engineer S Guide To MocDocumento5 pagineAn Engineer S Guide To MocAnonymous 1XHScfCI100% (1)
- Study and Improvement in Operations of Chemical Plant: Guide: Shri. Mahesh DhawalikarDocumento68 pagineStudy and Improvement in Operations of Chemical Plant: Guide: Shri. Mahesh DhawalikarPrathamesh NaikNessuna valutazione finora
- LECTURE - 03 - CDB 3044 - Conceptual Process Design - Synthesis of Reaction System (I)Documento29 pagineLECTURE - 03 - CDB 3044 - Conceptual Process Design - Synthesis of Reaction System (I)Ong Jia YeeNessuna valutazione finora
- Bhopal Disaster ReportDocumento1 paginaBhopal Disaster ReportshaniaNessuna valutazione finora
- Cpi PPT Enrollment No 10 To 13Documento32 pagineCpi PPT Enrollment No 10 To 13arshit5dobriyaNessuna valutazione finora
- Texas City Refinery Explosion ReportDocumento10 pagineTexas City Refinery Explosion ReportNimra JalilNessuna valutazione finora
- Green Chem Practical ValiDocumento15 pagineGreen Chem Practical ValiKomalpreet KaurNessuna valutazione finora
- Major Accidents in Oil and Gas, Petrochemicals Slide PresentationsDocumento16 pagineMajor Accidents in Oil and Gas, Petrochemicals Slide PresentationsAimi Saari100% (1)
- Group 1 - Section 01G - Separation Project PDFDocumento46 pagineGroup 1 - Section 01G - Separation Project PDFHatta AimanNessuna valutazione finora
- Bayer CropScience Runaway ReactionDocumento10 pagineBayer CropScience Runaway ReactionSatish JadhavNessuna valutazione finora
- Fire & Explosion During Tank Cleaning On A Chemical TankerDocumento4 pagineFire & Explosion During Tank Cleaning On A Chemical TankerHoàng Anh PhạmNessuna valutazione finora
- Bhopal Gas Tragedy Case StudyDocumento17 pagineBhopal Gas Tragedy Case StudyArijit PatiNessuna valutazione finora
- Principle 9 12Documento18 paginePrinciple 9 12taayush86Nessuna valutazione finora
- Background To Ioc FireDocumento7 pagineBackground To Ioc FirePratyaksh JainNessuna valutazione finora
- A Written Report in The: Introduction To Industrial ChemistryDocumento4 pagineA Written Report in The: Introduction To Industrial ChemistryJulius Supe-riorNessuna valutazione finora
- Top 27 Chemical Engineer Interview Questions and Answers - WiseStepDocumento7 pagineTop 27 Chemical Engineer Interview Questions and Answers - WiseStepAkash BodekarNessuna valutazione finora
- Bhopal LOPADocumento3 pagineBhopal LOPAFakhrul RaziNessuna valutazione finora
- Bhopal Gas Tragedy Case StudyDocumento12 pagineBhopal Gas Tragedy Case StudyMary Grace D. AlmiranezNessuna valutazione finora
- Synthesis of Tramadol LabDocumento3 pagineSynthesis of Tramadol Labchedhed50% (2)
- SANYO Semiconductor's Environmental ManagementDocumento6 pagineSANYO Semiconductor's Environmental ManagementDeign SeseNessuna valutazione finora
- Module 4Documento11 pagineModule 4yiyiyi7699Nessuna valutazione finora
- Bhopal PDFDocumento2 pagineBhopal PDFRatna Paramitha SariNessuna valutazione finora
- Prevent runaway phenol-formaldehyde reactionsDocumento6 paginePrevent runaway phenol-formaldehyde reactionsElena TodorovskaNessuna valutazione finora
- DIPLOMA IN OCCUPATIONAL SAFETY AND HEALTHDocumento10 pagineDIPLOMA IN OCCUPATIONAL SAFETY AND HEALTHsyukreenNessuna valutazione finora
- FA7 - Confined Space Case StudyDocumento7 pagineFA7 - Confined Space Case StudyaleanneNessuna valutazione finora
- Examples For Process SynthesisDocumento14 pagineExamples For Process SynthesisgoldflackNessuna valutazione finora
- Spe 123072Documento13 pagineSpe 123072Jose Gregorio Fariñas GagoNessuna valutazione finora
- Mechanical Properties of Polycarbonate: Experiment and Modeling for Aeronautical and Aerospace ApplicationsDa EverandMechanical Properties of Polycarbonate: Experiment and Modeling for Aeronautical and Aerospace ApplicationsNessuna valutazione finora
- Polyoxymethylene Handbook: Structure, Properties, Applications and their NanocompositesDa EverandPolyoxymethylene Handbook: Structure, Properties, Applications and their NanocompositesNessuna valutazione finora
- Recent Trends and Innovations in Sustainable Treatment Technologies for Heavy Metals, Dyes and Other XenobioticsDa EverandRecent Trends and Innovations in Sustainable Treatment Technologies for Heavy Metals, Dyes and Other XenobioticsNessuna valutazione finora
- Input FileDocumento10 pagineInput FileVipin NairNessuna valutazione finora
- X-1-Estimating Tool - Rev 0Documento10 pagineX-1-Estimating Tool - Rev 0Vipin NairNessuna valutazione finora
- Blackjack Cheat Sheet PDF Color PDFDocumento1 paginaBlackjack Cheat Sheet PDF Color PDFVipin NairNessuna valutazione finora
- Corsair 7 MIRs Feb 20 Feb 2717 NM 13 UsDocumento1 paginaCorsair 7 MIRs Feb 20 Feb 2717 NM 13 UsVipin NairNessuna valutazione finora
- Steel Cals SimpleDocumento53 pagineSteel Cals SimpleVashish RamrechaNessuna valutazione finora
- Circuitization Project Workflow GuideDocumento1 paginaCircuitization Project Workflow GuideVipin NairNessuna valutazione finora
- Stream Inspection Criteria FormDocumento4 pagineStream Inspection Criteria FormVipin NairNessuna valutazione finora
- DIY Cloth Face Covering Instructions PDFDocumento3 pagineDIY Cloth Face Covering Instructions PDFnathanNessuna valutazione finora
- 965 B10193 05,00Documento1 pagina965 B10193 05,00Vipin NairNessuna valutazione finora
- Texas MudHensDocumento1 paginaTexas MudHensVipin NairNessuna valutazione finora
- Xref Lines Not in LCI DBDocumento8 pagineXref Lines Not in LCI DBVipin NairNessuna valutazione finora
- CUI Project ExchnagersDocumento5 pagineCUI Project ExchnagersVipin NairNessuna valutazione finora
- Static Head Calculation For B-31Documento1 paginaStatic Head Calculation For B-31Vipin NairNessuna valutazione finora
- Terminal 3 Map2 - 2015 - R3 - tcm13-4102Documento2 pagineTerminal 3 Map2 - 2015 - R3 - tcm13-4102Vipin NairNessuna valutazione finora
- Sphere MAWPDocumento2 pagineSphere MAWPVipin NairNessuna valutazione finora
- Management of Critical Process Equipment To Ensure It Is Designed and Installed Correctly, and That It Operates and Is Maintained ProperlyDocumento2 pagineManagement of Critical Process Equipment To Ensure It Is Designed and Installed Correctly, and That It Operates and Is Maintained ProperlyVipin NairNessuna valutazione finora
- LWN TablesDocumento7 pagineLWN TablesVipin NairNessuna valutazione finora
- Vibration Related Failures of Small Bore AttachmentsDocumento13 pagineVibration Related Failures of Small Bore AttachmentsJose PradoNessuna valutazione finora
- Excel VBA For Dummies. BonusChapter02Documento4 pagineExcel VBA For Dummies. BonusChapter02nick_giannNessuna valutazione finora
- A-18 Top HeadDocumento1 paginaA-18 Top HeadVipin NairNessuna valutazione finora
- Redlined DWGDocumento1 paginaRedlined DWGVipin NairNessuna valutazione finora
- Pressure Vessel MI Field TemplateDocumento1 paginaPressure Vessel MI Field TemplateVipin NairNessuna valutazione finora
- E Battery TanksDocumento8 pagineE Battery TanksVipin NairNessuna valutazione finora
- College Engineering Commencement TicketDocumento1 paginaCollege Engineering Commencement TicketVipin NairNessuna valutazione finora
- PVElite Installation MethodDocumento1 paginaPVElite Installation MethodadnaniaziNessuna valutazione finora
- 60CSTL H2SDocumento2 pagine60CSTL H2SVipin NairNessuna valutazione finora
- 05 Minor Moc SDR FormDocumento23 pagine05 Minor Moc SDR FormVipin NairNessuna valutazione finora
- 15CSTL NaDocumento3 pagine15CSTL NaVipin NairNessuna valutazione finora
- 30S316 H2SDocumento2 pagine30S316 H2SVipin NairNessuna valutazione finora
- CTLS Interface Developers GuideDocumento242 pagineCTLS Interface Developers GuideLucas Pires SimãoNessuna valutazione finora
- Hospital Building Civil ProjectDocumento128 pagineHospital Building Civil ProjectArun Ragu100% (6)
- To Civil Engineering: RoadsDocumento30 pagineTo Civil Engineering: Roadshemant kumarNessuna valutazione finora
- Abstract Substructure Conc - Frame Westgate RealDocumento4 pagineAbstract Substructure Conc - Frame Westgate RealTashamiswa MajachaniNessuna valutazione finora
- Ansaldo Thomassen - Flexible Service Agreements (2014)Documento4 pagineAnsaldo Thomassen - Flexible Service Agreements (2014)guerrezNessuna valutazione finora
- KSSR - MatematikDocumento6 pagineKSSR - MatematikFaris FarhanNessuna valutazione finora
- DevelopmentThatPays ScrumToScrumban CheatSheet 2 - 0Documento1 paginaDevelopmentThatPays ScrumToScrumban CheatSheet 2 - 0tarikNessuna valutazione finora
- Ticketreissue PDFDocumento61 pagineTicketreissue PDFnicoNicoletaNessuna valutazione finora
- Feature Setup Description: Software Basic Data Mcs - TCBCDocumento77 pagineFeature Setup Description: Software Basic Data Mcs - TCBCAlexis MauricioNessuna valutazione finora
- Floor ManualDocumento35 pagineFloor ManualGihan ChathurangaNessuna valutazione finora
- HRIS1Documento24 pagineHRIS1UMESH VINAYAK ARVINDEKARNessuna valutazione finora
- Sch40 80 ASTM A53Documento2 pagineSch40 80 ASTM A53Keshia Murillo PinnockNessuna valutazione finora
- Learjet 45 Pilot Traning Manual Volumen 2Documento539 pagineLearjet 45 Pilot Traning Manual Volumen 2Agustin Bernales88% (8)
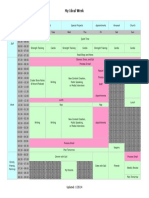
- My Ideal Week PDFDocumento1 paginaMy Ideal Week PDFAnonymous QE45TVC9e3Nessuna valutazione finora
- By Himanshu Panwar Asst. Prof. Civil Engineering Department AkgecDocumento34 pagineBy Himanshu Panwar Asst. Prof. Civil Engineering Department AkgecAlok0% (1)
- Co-Ordinated By: DR Parul Presented By: DR GurneetDocumento45 pagineCo-Ordinated By: DR Parul Presented By: DR Gurneetreenujohney100% (2)
- Multipoint Socket Profile VW 010 43: KonzernnormDocumento4 pagineMultipoint Socket Profile VW 010 43: KonzernnormRicardo Vitoriano100% (1)
- Insulation ProductsDocumento1 paginaInsulation ProductsDygoPalNessuna valutazione finora
- Specialized Epic EVO 2021Documento3 pagineSpecialized Epic EVO 2021MTB-VCONessuna valutazione finora
- Side Wall SprinklerDocumento6 pagineSide Wall SprinklerLasandu WanniarachchiNessuna valutazione finora
- VF1 Technicalspecifications 031997 EN PDFDocumento43 pagineVF1 Technicalspecifications 031997 EN PDFelectricistNessuna valutazione finora
- 1989 Volvo 740 Instruments and ControlsDocumento107 pagine1989 Volvo 740 Instruments and Controlsskyliner538Nessuna valutazione finora
- Project: Water Supply Layout Finals Drawn By: 20141142805 Date: 10/11/2018 Sheet No. 1 of 2Documento1 paginaProject: Water Supply Layout Finals Drawn By: 20141142805 Date: 10/11/2018 Sheet No. 1 of 2Jabber Reyes AmborNessuna valutazione finora
- Restaurant Pub VIP Lounge Camp Pune SaleDocumento4 pagineRestaurant Pub VIP Lounge Camp Pune SaleChandrashekhar Naikare0% (1)
- Casing & Compressor of Air ConditionerDocumento22 pagineCasing & Compressor of Air ConditionerAbdullah Zakirin Abdul 'AzamNessuna valutazione finora
- ACEEE - Best Practices For Data Centres - Lessons LearnedDocumento12 pagineACEEE - Best Practices For Data Centres - Lessons LearnedtonybudgeNessuna valutazione finora
- Sustainable Energy and Resource ManagementDocumento318 pagineSustainable Energy and Resource ManagementRajdeepSenNessuna valutazione finora
- Text Programming Guide For iOSDocumento106 pagineText Programming Guide For iOSPetr MánekNessuna valutazione finora
- Pyxis SPT HepDocumento597 paginePyxis SPT HepanithaarumallaNessuna valutazione finora
- I2C Bus ManualDocumento51 pagineI2C Bus Manualapi-26349602100% (6)