Potrebbero piacerti anche
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (121)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (588)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (400)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (266)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5794)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (345)
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (895)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- Clinical Cases in PsychiatryDocumento161 pagineClinical Cases in PsychiatryAna Roman100% (35)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- Proofreading: Basic Guide (Research)Documento34 pagineProofreading: Basic Guide (Research)Mary Christelle100% (1)
- Five Content Areas and Percent of Scored Test Items (Range) in Each AreaDocumento5 pagineFive Content Areas and Percent of Scored Test Items (Range) in Each Areaসোমনাথ মহাপাত্রNessuna valutazione finora
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- Din en 10346Documento45 pagineDin en 10346Lucero AlemanNessuna valutazione finora
- UWORLD Biostatistics Book Review PDFDocumento93 pagineUWORLD Biostatistics Book Review PDFসোমনাথ মহাপাত্র50% (2)
- Neuro Tract Lesions Ps230114Documento16 pagineNeuro Tract Lesions Ps230114সোমনাথ মহাপাত্রNessuna valutazione finora
- Learning Module 4 - BARTENDINGDocumento34 pagineLearning Module 4 - BARTENDINGivy mae flores67% (3)
- Case Study of AmoebiasisDocumento16 pagineCase Study of AmoebiasisGlorielle ElvambuenaNessuna valutazione finora
- Overall Merit List MD Ms Jan2018 PUBLDocumento440 pagineOverall Merit List MD Ms Jan2018 PUBLসোমনাথ মহাপাত্র0% (1)
- 1 SAP HCM Overview - IntroductionDocumento32 pagine1 SAP HCM Overview - IntroductionashwiniNessuna valutazione finora
- WWW Creativebloq Com Infographic Tools 2131971Documento20 pagineWWW Creativebloq Com Infographic Tools 2131971Martin_Arrieta_GNessuna valutazione finora
- Milling Machine Maintenance, Safety and OperationDocumento3 pagineMilling Machine Maintenance, Safety and OperationPPSwain100% (1)
- Openstack Deployment Ops Guide PDFDocumento197 pagineOpenstack Deployment Ops Guide PDFBinank PatelNessuna valutazione finora
- CBT 15 1029Documento13 pagineCBT 15 1029সোমনাথ মহাপাত্রNessuna valutazione finora
- 1201020895PL IMillerDocumento26 pagine1201020895PL IMillerসোমনাথ মহাপাত্রNessuna valutazione finora
- BD Biosciences Support - Protocols - Intracellular Staining of Human Red Blood CellsDocumento1 paginaBD Biosciences Support - Protocols - Intracellular Staining of Human Red Blood Cellsসোমনাথ মহাপাত্রNessuna valutazione finora
- Brandtzaeg 1981Documento14 pagineBrandtzaeg 1981সোমনাথ মহাপাত্রNessuna valutazione finora
- Chapter 3 Haemoglobin Pattern Analysis: 3.1. Chromatographic Methods (For Hba Determination)Documento27 pagineChapter 3 Haemoglobin Pattern Analysis: 3.1. Chromatographic Methods (For Hba Determination)সোমনাথ মহাপাত্রNessuna valutazione finora
- 149 FullDocumento10 pagine149 Fullসোমনাথ মহাপাত্রNessuna valutazione finora
- Immune Recognition of Self Nucleic Acids Driven by Endogenous Antimicrobial Peptides: Role in AutoimmunityDocumento176 pagineImmune Recognition of Self Nucleic Acids Driven by Endogenous Antimicrobial Peptides: Role in Autoimmunityসোমনাথ মহাপাত্রNessuna valutazione finora
- Boards and Beyound Step 2 Cs PalpitationsDocumento4 pagineBoards and Beyound Step 2 Cs Palpitationsসোমনাথ মহাপাত্রNessuna valutazione finora
- Account Statement As of 04-05-2020 19:48:27 GMT +0530Documento11 pagineAccount Statement As of 04-05-2020 19:48:27 GMT +0530সোমনাথ মহাপাত্রNessuna valutazione finora
- Cell-Cell Interactions: Concept OutlineDocumento18 pagineCell-Cell Interactions: Concept Outlineসোমনাথ মহাপাত্রNessuna valutazione finora
- DHR-ICMR Funded Workshops FormatDocumento3 pagineDHR-ICMR Funded Workshops Formatসোমনাথ মহাপাত্রNessuna valutazione finora
- Icmr Talent FormDocumento2 pagineIcmr Talent Formসোমনাথ মহাপাত্রNessuna valutazione finora
- Griffin Observership ApplicationDocumento7 pagineGriffin Observership Applicationসোমনাথ মহাপাত্রNessuna valutazione finora
- Observership Application ST - VincentsDocumento2 pagineObservership Application ST - Vincentsসোমনাথ মহাপাত্রNessuna valutazione finora
- Visiting Scholar ChecklistDocumento9 pagineVisiting Scholar Checklistসোমনাথ মহাপাত্রNessuna valutazione finora
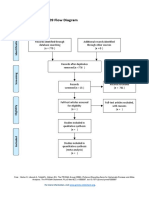
- PRISMA 2009 Flow Diagram PDFDocumento1 paginaPRISMA 2009 Flow Diagram PDFসোমনাথ মহাপাত্রNessuna valutazione finora
- ElectivesDocumento5 pagineElectivesসোমনাথ মহাপাত্র100% (1)
- Professional Education: St. Louis Review Center, IncDocumento10 pagineProfessional Education: St. Louis Review Center, IncEarshad Shinichi IIINessuna valutazione finora
- Comparative Analysis of Motivation TheoriesDocumento14 pagineComparative Analysis of Motivation TheoriesNomvelo MajolaNessuna valutazione finora
- Content Kartilya NG Katipunan: Kataastaasan, Kagalanggalangang Katipunan NG Mga Anak NG Bayan)Documento6 pagineContent Kartilya NG Katipunan: Kataastaasan, Kagalanggalangang Katipunan NG Mga Anak NG Bayan)AngelaNessuna valutazione finora
- Police Forces and The Administration of Justice in Tanzania.Documento6 paginePolice Forces and The Administration of Justice in Tanzania.Praygod Manase100% (2)
- Checklist-Telephone - Mobile ExpenseDocumento2 pagineChecklist-Telephone - Mobile ExpenseMichelle Domanacal UrsabiaNessuna valutazione finora
- The Appropriate Biochemical Oxygen Demand Concentration For Designing Domestic Wastewater Treatment PlantDocumento8 pagineThe Appropriate Biochemical Oxygen Demand Concentration For Designing Domestic Wastewater Treatment PlantabdulNessuna valutazione finora
- Jobsheet PMDocumento49 pagineJobsheet PMwindhy fitrianaNessuna valutazione finora
- Buyer Behavior ModelDocumento1 paginaBuyer Behavior ModelraihanulhasanNessuna valutazione finora
- Dialogue-2: Problem of Our CountryDocumento6 pagineDialogue-2: Problem of Our CountrysiamNessuna valutazione finora
- CALDER New Research On Low-Frequency Membrane AbsorbersDocumento11 pagineCALDER New Research On Low-Frequency Membrane AbsorbersAndre VareNessuna valutazione finora
- SSP 861603 - EN - Tire Pressure Monitoring SystemsDocumento42 pagineSSP 861603 - EN - Tire Pressure Monitoring Systemsa.diedrichsNessuna valutazione finora
- Project Proposal Environmental Protection Program-DeNRDocumento57 pagineProject Proposal Environmental Protection Program-DeNRLGU PadadaNessuna valutazione finora
- Lesson 11Documento3 pagineLesson 11Jhoanna Rose AlingalanNessuna valutazione finora
- Wavoo Wajeeha Women's College - Annual Report - 2013-14Documento29 pagineWavoo Wajeeha Women's College - Annual Report - 2013-14kayalonthewebNessuna valutazione finora
- Statistics and Data CollectionDocumento11 pagineStatistics and Data CollectionRichimon LicerioNessuna valutazione finora
- Cooper - Formal Review of Karla Noles RaDocumento6 pagineCooper - Formal Review of Karla Noles RaMark CooperNessuna valutazione finora
- Neighbor'S Plot - : Sheet No Rev No R0Documento1 paginaNeighbor'S Plot - : Sheet No Rev No R0jibeesh cmNessuna valutazione finora
- The Brain in Your Pocket Evidence - That - SDocumento8 pagineThe Brain in Your Pocket Evidence - That - Sanwaarft123Nessuna valutazione finora
- HCT Baniqued P.D.E. Paper1 Version3 FullpaperDocumento8 pagineHCT Baniqued P.D.E. Paper1 Version3 FullpaperJoshua HernandezNessuna valutazione finora
- Region XiDocumento2 pagineRegion XiGarcia, Rafael Rico O.Nessuna valutazione finora
- New Rich Text DocumentDocumento12 pagineNew Rich Text Documentsonam dorjiNessuna valutazione finora
- Mico - Hydraulic Power Brake Systems For ForkliftsDocumento4 pagineMico - Hydraulic Power Brake Systems For ForkliftsJenner Volnney Quispe Chata100% (1)