Potrebbero piacerti anche
- Advanced Medicine Recall A Must For MRCP PDFDocumento712 pagineAdvanced Medicine Recall A Must For MRCP PDFKai Xin100% (2)
- Paces Exam Cases 2nd Version PDFDocumento471 paginePaces Exam Cases 2nd Version PDFMuntadher Kareem100% (1)
- (Get Now) SOAP For Family Medicine by Daniel Maldonado: Â Š PDF Â Š KINDLE Â ŠDocumento12 pagine(Get Now) SOAP For Family Medicine by Daniel Maldonado: Â Š PDF Â Š KINDLE Â ŠMauricio Solano DiazNessuna valutazione finora
- PEAC OphthalmologyDocumento45 paginePEAC OphthalmologySdNessuna valutazione finora
- MIMS Summary Table-G6PDDocumento1 paginaMIMS Summary Table-G6PDenchanteresse100% (3)
- 2017-2018 Intern GuideDocumento31 pagine2017-2018 Intern GuideaskjagNessuna valutazione finora
- Internal Medicine A Guide To Clinical Therapeutics by Rebecca L Attridge Monica L Miller Rebecca Moote Laurajo Ryan 0071745807Documento5 pagineInternal Medicine A Guide To Clinical Therapeutics by Rebecca L Attridge Monica L Miller Rebecca Moote Laurajo Ryan 0071745807Hesbon MomanyiNessuna valutazione finora
- CMPA Handbook For PhysiciansDocumento56 pagineCMPA Handbook For Physiciansteena6506763Nessuna valutazione finora
- Data Interpretation For Medical StudentDocumento18 pagineData Interpretation For Medical StudentWee K WeiNessuna valutazione finora
- Nephrotic and Nephritic Syndrome GuideDocumento3 pagineNephrotic and Nephritic Syndrome Guidewinston1234Nessuna valutazione finora
- EMRA EMS EssentialsDocumento167 pagineEMRA EMS EssentialsMiko Ramoso100% (3)
- IMCIDocumento112 pagineIMCIJohann Dexter Malimban GloriosoNessuna valutazione finora
- SABER IM PrometricDocumento71 pagineSABER IM Prometricisra zaidNessuna valutazione finora
- Common Cold AAFPDocumento7 pagineCommon Cold AAFPAnonymous so6ZnlKywNessuna valutazione finora
- SOAP Note TemplateDocumento1 paginaSOAP Note Templatenmb1986Nessuna valutazione finora
- Anesthesiology GuideDocumento4 pagineAnesthesiology GuideGeorge Wang100% (1)
- List of 136 CCS cases from Feb 2020Documento4 pagineList of 136 CCS cases from Feb 2020Ramanpreet Kaur MaanNessuna valutazione finora
- Ckform 7Documento21 pagineCkform 7walt65100% (1)
- Ethics Uworld NotesDocumento3 pagineEthics Uworld NotesActeen MyoseenNessuna valutazione finora
- Primer To IM ClerkshipDocumento37 paginePrimer To IM Clerkshipjcraja100% (1)
- Blood and Drugs Medicine NotesDocumento39 pagineBlood and Drugs Medicine Notesrahuul prasadNessuna valutazione finora
- History and Physical Exam TemplateDocumento3 pagineHistory and Physical Exam TemplatederekcftamNessuna valutazione finora
- Deconstructing The ECG Curve - The Components of The Tracing: Key ConceptsDocumento117 pagineDeconstructing The ECG Curve - The Components of The Tracing: Key ConceptsdrynwhylNessuna valutazione finora
- Pediatrics - Lower AirwayDocumento3 paginePediatrics - Lower AirwayJasmine KangNessuna valutazione finora
- Usmle Step 2 CsDocumento70 pagineUsmle Step 2 CsAlvi MuldaniNessuna valutazione finora
- Residency Interview QuestionsDocumento3 pagineResidency Interview QuestionsLujain Al OmariNessuna valutazione finora
- Hepatorenal Syndrome, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsDa EverandHepatorenal Syndrome, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNessuna valutazione finora
- History and physical assessment guideDocumento31 pagineHistory and physical assessment guideShalini RavNessuna valutazione finora
- YFT IM Notes 1Documento100 pagineYFT IM Notes 1AHMAD ALROWAILYNessuna valutazione finora
- Biostats and Epi-UworldDocumento3 pagineBiostats and Epi-UworldMikeRSteinNessuna valutazione finora
- Hemodynamics Basic Concepts 1204053445109897 4Documento115 pagineHemodynamics Basic Concepts 1204053445109897 4valeriesolidum100% (1)
- PANCE Prep Pearls Valvular Disease PDFDocumento4 paginePANCE Prep Pearls Valvular Disease PDFkatNessuna valutazione finora
- CaRMS Guide: The Application ProcessDocumento26 pagineCaRMS Guide: The Application Processbicodoc100% (1)
- Onlinemeded Notes CardioDocumento1 paginaOnlinemeded Notes CardioCourtney HolbrookNessuna valutazione finora
- Gynecology StudyguideDocumento39 pagineGynecology StudyguideGameron777Nessuna valutazione finora
- Ob GynDocumento4 pagineOb GynAstariAnnemarieNessuna valutazione finora
- Mediwood 3.0 by DR Naveen Koval (With Links)Documento707 pagineMediwood 3.0 by DR Naveen Koval (With Links)Rahul B100% (1)
- The AOA Guide: How To Succeed Inthe3 Year Clerkships: Example Notes For The MsiiiDocumento20 pagineThe AOA Guide: How To Succeed Inthe3 Year Clerkships: Example Notes For The Msiiinybiker100% (1)
- QTc Interval - The Corrected QT IntervalDocumento4 pagineQTc Interval - The Corrected QT IntervalkaelenNessuna valutazione finora
- CCT - CCI Code of EthicsDocumento2 pagineCCT - CCI Code of EthicsAvanca LouisNessuna valutazione finora
- NeurologyDocumento4 pagineNeurologyClaudioAhumadaNessuna valutazione finora
- ECG Interpretation DR - Rawan AlshreemDocumento25 pagineECG Interpretation DR - Rawan AlshreemMarymii Al-sahlawiiNessuna valutazione finora
- A. Subjective: 1. Progress NoteDocumento3 pagineA. Subjective: 1. Progress NoteEvan100% (1)
- High Yield SurgeryDocumento77 pagineHigh Yield SurgeryDr.2020Nessuna valutazione finora
- Lung PathologyDocumento101 pagineLung Pathologyhm3398Nessuna valutazione finora
- Gynecology and ObstetricsvvvvvvvvvvvvvvvvvvvvvvvvvvvvvvvvvvvvvvvvvDocumento133 pagineGynecology and ObstetricsvvvvvvvvvvvvvvvvvvvvvvvvvvvvvvvvvvvvvvvvvȚurcan IurieNessuna valutazione finora
- Md2017 Carms Mock Interview GuideDocumento6 pagineMd2017 Carms Mock Interview GuideLizamna ReynosoNessuna valutazione finora
- Step 1 UW Objectives Subjectwise 2022Documento474 pagineStep 1 UW Objectives Subjectwise 2022saranya sankarNessuna valutazione finora
- History Taking - Chief Complaint, HPI, PMH, FH, SHDocumento52 pagineHistory Taking - Chief Complaint, HPI, PMH, FH, SHGurpreet CharaNessuna valutazione finora
- DeVirglio NotesDocumento77 pagineDeVirglio NotesAlvand SehatNessuna valutazione finora
- Aquifer InternalMedicine09 - 55Documento7 pagineAquifer InternalMedicine09 - 55JulieNessuna valutazione finora
- Asthma Review PDFDocumento12 pagineAsthma Review PDFdanielc503Nessuna valutazione finora
- Amboss Hemolytic AnemiaDocumento16 pagineAmboss Hemolytic AnemiaAhmed Ali100% (2)
- Differential Diagnosis of Valvular Heart DiseaseDocumento10 pagineDifferential Diagnosis of Valvular Heart DiseaseAbhisek ChatterjeeNessuna valutazione finora
- Kaplan Pharmacology FlashcardsDocumento2 pagineKaplan Pharmacology Flashcardsoussama dieselNessuna valutazione finora
- Guidelines For Writing CVDocumento1 paginaGuidelines For Writing CVanwar933Nessuna valutazione finora
- Rosh ReviewsDocumento19 pagineRosh ReviewsTracy NwanneNessuna valutazione finora
- Principles of ECGDocumento11 paginePrinciples of ECGDeinielle Magdangal RomeroNessuna valutazione finora
- Internal Med TipsDocumento2 pagineInternal Med TipsNick100% (1)
- Interview Questions 2016 Draft Version 7-18-16Documento6 pagineInterview Questions 2016 Draft Version 7-18-16Sisca Dwi AgustinaNessuna valutazione finora
- Objectives IMDocumento104 pagineObjectives IMlaraNessuna valutazione finora
- JournalDocumento6 pagineJournalMiko RamosoNessuna valutazione finora
- PSMID Polio Statement - SEP23, 2019 - FinalDocumento4 paginePSMID Polio Statement - SEP23, 2019 - FinalMiko RamosoNessuna valutazione finora
- PSMID Polio Statement - SEP23, 2019 - FinalDocumento4 paginePSMID Polio Statement - SEP23, 2019 - FinalMiko RamosoNessuna valutazione finora
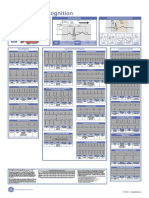
- Poster1 Arrhythmia Recognition e PDFDocumento1 paginaPoster1 Arrhythmia Recognition e PDFMiko RamosoNessuna valutazione finora
- PRISMA 2009 Flow Diagram PDFDocumento1 paginaPRISMA 2009 Flow Diagram PDFKalis WarenNessuna valutazione finora
- Emailing CPG-E PDFDocumento206 pagineEmailing CPG-E PDFCarlos H. AcuñaNessuna valutazione finora
- Truly HomeDocumento1 paginaTruly HomeMiko RamosoNessuna valutazione finora
- Song ListDocumento5 pagineSong ListMiko RamosoNessuna valutazione finora
- Legal MedicineDocumento2 pagineLegal MedicineMiko RamosoNessuna valutazione finora
- ZKG IndiaDocumento36 pagineZKG Indiajoe_kudo0% (1)
- Physics Mtmar - EdoneDocumento1 paginaPhysics Mtmar - EdoneAllan Estrada BasugaNessuna valutazione finora
- Electropneumatic and Hydraulic DNT241: Experiment No. 4Documento7 pagineElectropneumatic and Hydraulic DNT241: Experiment No. 4Izz Hanzalah AhmadNessuna valutazione finora
- Gating System Design GuideDocumento11 pagineGating System Design GuideAshok Pradhan100% (1)
- Application of The Giroud - Han Design Method For Geosynthetic Reinforced Unpaved Roads With Tencate Mirafi GeosyntheticsDocumento7 pagineApplication of The Giroud - Han Design Method For Geosynthetic Reinforced Unpaved Roads With Tencate Mirafi GeosyntheticsFaten Abou ShakraNessuna valutazione finora
- Unit & DimensionsDocumento9 pagineUnit & DimensionsRandhir SinghNessuna valutazione finora
- Swarmalators Under Competitive Time-Varying Phase InteractionsDocumento21 pagineSwarmalators Under Competitive Time-Varying Phase Interactionsim.marzaNessuna valutazione finora
- Unit 1 Test ReviewDocumento4 pagineUnit 1 Test Reviewandrew culkinNessuna valutazione finora
- CIS221-Design of Concrete Structures: BY Dr. Abdallah MostafaDocumento20 pagineCIS221-Design of Concrete Structures: BY Dr. Abdallah Mostafamagdy makramNessuna valutazione finora
- Package Insert - PYROSPERSE™ Dispersing Agent (English) - Original - 27876Documento7 paginePackage Insert - PYROSPERSE™ Dispersing Agent (English) - Original - 27876Putri DozanNessuna valutazione finora
- Heater DetailsDocumento35 pagineHeater DetailsPushkar Pandit100% (1)
- CFD Application Tutorials 2Documento35 pagineCFD Application Tutorials 2Jubril AkinwandeNessuna valutazione finora
- RT60 Reverberation TimeDocumento21 pagineRT60 Reverberation TimeDinushaNessuna valutazione finora
- EOR Screening Part 2 Taber-MartinDocumento7 pagineEOR Screening Part 2 Taber-MartinPerwira HandhikoNessuna valutazione finora
- Work Sheet IDocumento5 pagineWork Sheet IgrmdrjNessuna valutazione finora
- Ageing of Zinc Alloys: January 2011Documento23 pagineAgeing of Zinc Alloys: January 2011Alicia Jara ChavezNessuna valutazione finora
- Dowf Rost: Engineering and Operating GuideDocumento44 pagineDowf Rost: Engineering and Operating GuidehamishlewisNessuna valutazione finora
- A Ghost in The MachineDocumento7 pagineA Ghost in The MachineSicklslicerNessuna valutazione finora
- CBSE Class 12 Chemistry Sample Paper-15: Material Downloaded From - 1 / 14Documento14 pagineCBSE Class 12 Chemistry Sample Paper-15: Material Downloaded From - 1 / 14Allen Neal JonesNessuna valutazione finora
- Experiment No. 1 Objective: Vernier Callipers, A Spherical Body (It Can Be A Pendulum Bob), A Beaker or A CalorimeterDocumento2 pagineExperiment No. 1 Objective: Vernier Callipers, A Spherical Body (It Can Be A Pendulum Bob), A Beaker or A CalorimeterShivam YadavNessuna valutazione finora
- Sample Calculus Problems: Single Variable FunctionsDocumento155 pagineSample Calculus Problems: Single Variable Functionsmoustafa.mehanna7564Nessuna valutazione finora
- Passive Flow Separation Control Over NACA 63018Documento1 paginaPassive Flow Separation Control Over NACA 63018miladrakhshaNessuna valutazione finora
- GulfSea Diesel GE 40 PDFDocumento2 pagineGulfSea Diesel GE 40 PDFObydur RahmanNessuna valutazione finora
- Literature Pressure GaugesDocumento5 pagineLiterature Pressure GaugesHardik AcharyaNessuna valutazione finora
- Simple and Inexpensive Microforge: by G. HilsonDocumento5 pagineSimple and Inexpensive Microforge: by G. Hilsonfoober123Nessuna valutazione finora
- .Fraunhofer - Diffraction.at - The.slit.Documento6 pagine.Fraunhofer - Diffraction.at - The.slit.NCHE BORISNessuna valutazione finora
- Geosynthetic Institute: GRI Test Method GM19Documento12 pagineGeosynthetic Institute: GRI Test Method GM19HeiderHuertaNessuna valutazione finora
- KSPDocumento12 pagineKSPSyaefudinNessuna valutazione finora
- Analysis of The Light J 3 Mesons in QCD Sum RulesDocumento11 pagineAnalysis of The Light J 3 Mesons in QCD Sum Rulesubik59Nessuna valutazione finora
- 3ap1 FG: High-Voltage Circuit-BreakerDocumento2 pagine3ap1 FG: High-Voltage Circuit-BreakerFernando VacaNessuna valutazione finora