Potrebbero piacerti anche
- Cima BP Plan Stakeholder EvaluationsDocumento6 pagineCima BP Plan Stakeholder Evaluationsapi-320921814Nessuna valutazione finora
- Research Lo 4 Research PaperDocumento16 pagineResearch Lo 4 Research Paperapi-320921814Nessuna valutazione finora
- Lo4 Lguilford JT Comments RevisedDocumento3 pagineLo4 Lguilford JT Comments Revisedapi-320921814Nessuna valutazione finora
- Lo1 Lguilford JT Comments RevisedDocumento3 pagineLo1 Lguilford JT Comments Revisedapi-320921814Nessuna valutazione finora
- Macro Artifact Lo2 Pufas and CRPDocumento18 pagineMacro Artifact Lo2 Pufas and CRPapi-320921814Nessuna valutazione finora
- Lguilford Lo7 FinalDocumento3 pagineLguilford Lo7 Finalapi-320921814Nessuna valutazione finora
- Ic Artifact Lo1 Group ProjectDocumento15 pagineIc Artifact Lo1 Group Projectapi-320921814Nessuna valutazione finora
- Micro Arifact Lo2 Case Study Write UpDocumento5 pagineMicro Arifact Lo2 Case Study Write Upapi-320921814Nessuna valutazione finora
- L Guilford 2016 ResumeDocumento4 pagineL Guilford 2016 Resumeapi-320921814Nessuna valutazione finora
- Lguilford Lo3 JT Comments RevisedDocumento3 pagineLguilford Lo3 JT Comments Revisedapi-320921814Nessuna valutazione finora
- Lguilford Lo2 FinalDocumento3 pagineLguilford Lo2 Finalapi-320921814Nessuna valutazione finora
- Lguilford Reflective SummaryDocumento2 pagineLguilford Reflective Summaryapi-320921814Nessuna valutazione finora
- Ksu Artifact Lo 8 Eval1Documento1 paginaKsu Artifact Lo 8 Eval1api-320921814Nessuna valutazione finora
- Laurenda Guilfords EvaluationDocumento4 pagineLaurenda Guilfords Evaluationapi-320921814Nessuna valutazione finora
- L Guilford EvalDocumento2 pagineL Guilford Evalapi-320921814Nessuna valutazione finora
- CCSD Artifact 6 Plate Waste StudyDocumento6 pagineCCSD Artifact 6 Plate Waste Studyapi-320921814Nessuna valutazione finora
- L Guilford Grady Critical EvalDocumento4 pagineL Guilford Grady Critical Evalapi-320921814Nessuna valutazione finora
- Health Policy Artifact Lo 7 AssignmentDocumento3 pagineHealth Policy Artifact Lo 7 Assignmentapi-320921814Nessuna valutazione finora
- Cima Artifact Lo3 Desc of SvcsDocumento4 pagineCima Artifact Lo3 Desc of Svcsapi-320921814Nessuna valutazione finora
- Harvard School of Public Health ArticleDocumento1 paginaHarvard School of Public Health Articleapi-320921814Nessuna valutazione finora
- Lguilford Lo5 FinalDocumento3 pagineLguilford Lo5 Finalapi-320921814Nessuna valutazione finora
- Lguilford 8 FinalDocumento4 pagineLguilford 8 Finalapi-320921814Nessuna valutazione finora
- L Guilford Introphil Portfolio FinalDocumento3 pagineL Guilford Introphil Portfolio Finalapi-320921814Nessuna valutazione finora
- Lguilford Lo6 FinalDocumento11 pagineLguilford Lo6 Finalapi-320921814Nessuna valutazione finora
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (894)
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (265)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (73)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (119)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- A5 SHARAN Health Participant Booklet NewDocumento70 pagineA5 SHARAN Health Participant Booklet NewJanaki KothariNessuna valutazione finora
- Urginea Indica Plant SummaryDocumento10 pagineUrginea Indica Plant Summaryv.k. yadavNessuna valutazione finora
- Genetic Analyses of Bolting in Bulb Onion Allium CepaDocumento10 pagineGenetic Analyses of Bolting in Bulb Onion Allium CepaManuel VegasNessuna valutazione finora
- Factsheet ABSF Spices, Herbs and AromaticsDocumento16 pagineFactsheet ABSF Spices, Herbs and AromaticsadNessuna valutazione finora
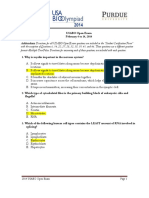
- USABO 14 Open Exam Final AnsDocumento16 pagineUSABO 14 Open Exam Final AnsGuest SuiteNessuna valutazione finora
- How Organisms ReproduceDocumento2 pagineHow Organisms ReproduceAnita GargNessuna valutazione finora
- Date Farming GuidelinesDocumento8 pagineDate Farming GuidelinesSubhiah CNessuna valutazione finora
- Ethnicraft 2012Documento75 pagineEthnicraft 2012witsgNessuna valutazione finora
- Preventing The Browning of Sliced FruitDocumento12 paginePreventing The Browning of Sliced FruitCYNTHIA100% (1)
- Isolation of Berberine From Berberis VulgarisDocumento6 pagineIsolation of Berberine From Berberis VulgarisArieNessuna valutazione finora
- DLL - Epp 6 - Q1 - W3Documento7 pagineDLL - Epp 6 - Q1 - W3Merlie Agtina Salamangkit-OlaloNessuna valutazione finora
- RepaHeel Beeswax-Based Gel For Treating Heel Spurs Has Been Produced in EUDocumento2 pagineRepaHeel Beeswax-Based Gel For Treating Heel Spurs Has Been Produced in EUPR.comNessuna valutazione finora
- Gundelia 2012cDocumento8 pagineGundelia 2012cIsmail Bazly ZarirNessuna valutazione finora
- Personal Vault - LNKDocumento18 paginePersonal Vault - LNKManushree NNessuna valutazione finora
- Seed GerminationDocumento26 pagineSeed Germinationnozel77Nessuna valutazione finora
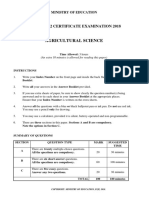
- 18 FY12 CEAgricultural Science QPDocumento13 pagine18 FY12 CEAgricultural Science QPSelina VuninaiNessuna valutazione finora
- Seed DormancyDocumento27 pagineSeed DormancyPayushni BhuyanNessuna valutazione finora
- 909 Symptoms and Treatment of Manganese Deficiency SplitDocumento6 pagine909 Symptoms and Treatment of Manganese Deficiency SplitazirNessuna valutazione finora
- 2002 Cacti Biology and Uses PDFDocumento291 pagine2002 Cacti Biology and Uses PDFReislaNessuna valutazione finora
- Pharmaceutical Sciences: A Study On Synergestic Wound Healing Activity of Capsicum and Pigeon PeaDocumento4 paginePharmaceutical Sciences: A Study On Synergestic Wound Healing Activity of Capsicum and Pigeon PeaBaru Chandrasekhar RaoNessuna valutazione finora
- Golden Apple Snails ManagementDocumento32 pagineGolden Apple Snails ManagementMaria Ric100% (1)
- Fungi Characteristics and ClassificationDocumento2 pagineFungi Characteristics and ClassificationRia AlcantaraNessuna valutazione finora
- Antioxidant Capacity of The Mediterranean Diet SAURA CALIXTO PDFDocumento6 pagineAntioxidant Capacity of The Mediterranean Diet SAURA CALIXTO PDFjoelNessuna valutazione finora
- Benefits of Functional DrinksDocumento22 pagineBenefits of Functional DrinksMoshmi MazumdarNessuna valutazione finora
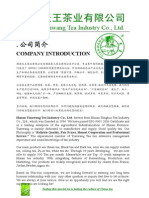
- New Green Tea CatalogDocumento9 pagineNew Green Tea CatalogSteveihNessuna valutazione finora
- Success Story of Sukhdev MaharajDocumento3 pagineSuccess Story of Sukhdev MaharajNeha SahuNessuna valutazione finora
- Sturtevants Notes On Edible Plants, Vol.2Documento704 pagineSturtevants Notes On Edible Plants, Vol.2Van_Kiser100% (1)
- Homeopathy & Ayurvedic Medicine: A Study On The Plants Used As ChopachiniDocumento4 pagineHomeopathy & Ayurvedic Medicine: A Study On The Plants Used As ChopachiniMillenium AyurvedaNessuna valutazione finora
- Therapeutic Diet V3Documento40 pagineTherapeutic Diet V3Aman Chvarsha100% (1)
- The Doctrine of SignaturesDocumento5 pagineThe Doctrine of SignaturesJoko RinantoNessuna valutazione finora