Potrebbero piacerti anche
- Congenital Glaucomas: 1. Primary 2. Iridocorneal DysgenesisDocumento12 pagineCongenital Glaucomas: 1. Primary 2. Iridocorneal DysgenesisChintya Nur FaizahNessuna valutazione finora
- Apoptosis (Kuliah) 2012Documento90 pagineApoptosis (Kuliah) 2012Chintya Nur FaizahNessuna valutazione finora
- Haldol Vs Paliperidon JAMA 05 2014Documento9 pagineHaldol Vs Paliperidon JAMA 05 2014Chintya Nur FaizahNessuna valutazione finora
- 2016 Article 1432Documento8 pagine2016 Article 1432Chintya Nur FaizahNessuna valutazione finora
- Clinical Pathology Course Handbook 2006-2009Documento57 pagineClinical Pathology Course Handbook 2006-2009hhchiuNessuna valutazione finora
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5794)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (344)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (587)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (73)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (265)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2219)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (119)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- Lesson Plan: Lesson: Carboxylic Acids (II)Documento3 pagineLesson Plan: Lesson: Carboxylic Acids (II)MarcTnnNessuna valutazione finora
- Finance & Account Executive with 6+ years of SAP FICO experienceDocumento3 pagineFinance & Account Executive with 6+ years of SAP FICO experienceSHIVANANDNessuna valutazione finora
- Pew CatalogsDocumento25 paginePew CatalogsBon HarperNessuna valutazione finora
- All About TransformersDocumento141 pagineAll About TransformersMy Transformers GuideNessuna valutazione finora
- InfraredDocumento9 pagineInfraredPaculba Louigi IgdonNessuna valutazione finora
- Iloilo City Regulation Ordinance 2016-095Documento3 pagineIloilo City Regulation Ordinance 2016-095Iloilo City CouncilNessuna valutazione finora
- Visual CPPDocumento23 pagineVisual CPPAnish SukumarNessuna valutazione finora
- Mechanics of breathing explained in 69 wordsDocumento18 pagineMechanics of breathing explained in 69 wordsZaliaSubplace S5357Nessuna valutazione finora
- in What Situation Does Alison Believe Facebook Users Might Abandon The Company?Documento10 paginein What Situation Does Alison Believe Facebook Users Might Abandon The Company?Lê TùngNessuna valutazione finora
- Đề Ôn Thi Kỳ 1 - Test 1Documento5 pagineĐề Ôn Thi Kỳ 1 - Test 1Thuỳ Dương NguyễnNessuna valutazione finora
- Mal Wares ListDocumento13 pagineMal Wares ListAditya SinghNessuna valutazione finora
- SteelTubeHandbook February2012Documento120 pagineSteelTubeHandbook February2012Adisak AumpiemNessuna valutazione finora
- Geometry by Total GadhaDocumento5 pagineGeometry by Total GadhaAarush JainNessuna valutazione finora
- Ffu 0001115 01Documento38 pagineFfu 0001115 01Karunia LestariNessuna valutazione finora
- The Caring TeachersDocumento43 pagineThe Caring TeachersCyruzLeyteNessuna valutazione finora
- DG Khan development schemes tender detailsDocumento9 pagineDG Khan development schemes tender detailsYousaf Khalid KhaulaNessuna valutazione finora
- Lex Sheers Multi Phase Meters Day 1Documento81 pagineLex Sheers Multi Phase Meters Day 1candra100% (5)
- Gábor Békés, Gábor Kézdi - Data Analysis For Business, Economics, and Policy-Cambridge University Press (2021)Documento742 pagineGábor Békés, Gábor Kézdi - Data Analysis For Business, Economics, and Policy-Cambridge University Press (2021)gatitahanyou100% (2)
- Mobile trading app features study during pandemicDocumento7 pagineMobile trading app features study during pandemicKomal YadavNessuna valutazione finora
- CARIBBEANDocumento15 pagineCARIBBEANAndrew NepomucenoNessuna valutazione finora
- Implementing Ipv6 in The Enterprise Network: CCNP Route: Implementing Ip RoutingDocumento109 pagineImplementing Ipv6 in The Enterprise Network: CCNP Route: Implementing Ip RoutingMed ArefNessuna valutazione finora
- Pump DrawingDocumento1 paginaPump DrawingOcta RioNessuna valutazione finora
- Absolac MSDSDocumento8 pagineAbsolac MSDSwitnwisdumb100% (1)
- Io ModuleDocumento11 pagineIo ModuleMichael Kent Gamon100% (2)
- CPI Genware ManualDocumento56 pagineCPI Genware ManualТимур ТамбиевNessuna valutazione finora
- Fire Hose Reel DimensionDocumento1 paginaFire Hose Reel DimensionChristianNessuna valutazione finora
- (TATA) NEXON Infotainment ManualDocumento173 pagine(TATA) NEXON Infotainment ManualZaman AliNessuna valutazione finora
- Bronze SAE 40Documento2 pagineBronze SAE 40fahazumeeNessuna valutazione finora
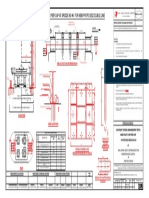
- Ohe Mast Fixing Arrangement On Pier Cap at Bridge No:46 For New Proposed Double LineDocumento1 paginaOhe Mast Fixing Arrangement On Pier Cap at Bridge No:46 For New Proposed Double LineRVNLPKG6B VBL-GTLMNessuna valutazione finora