Potrebbero piacerti anche
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (895)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (344)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (121)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- Answer Key: Introduction To Clinical CodingDocumento101 pagineAnswer Key: Introduction To Clinical Codingthamizh555100% (1)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (73)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- Course Pack L1Documento88 pagineCourse Pack L1Ernesto Hernandez-TrejoNessuna valutazione finora
- CataractDocumento45 pagineCataractAmit Martin100% (2)
- Water Seal DrainageDocumento6 pagineWater Seal DrainageAmit MartinNessuna valutazione finora
- Wound Care: Types of DressingDocumento5 pagineWound Care: Types of DressingAmit MartinNessuna valutazione finora
- Glasgow Coma Scale: Presented by Mr. Amit MartinDocumento58 pagineGlasgow Coma Scale: Presented by Mr. Amit MartinAmit MartinNessuna valutazione finora
- Retinal DetachmentDocumento51 pagineRetinal DetachmentAmit MartinNessuna valutazione finora
- Glasgow Coma Scale: Presented by Mr. Amit MartinDocumento58 pagineGlasgow Coma Scale: Presented by Mr. Amit MartinAmit MartinNessuna valutazione finora
- Wound CareDocumento4 pagineWound CareAmit MartinNessuna valutazione finora
- Sitz Bath: ObjectivesDocumento3 pagineSitz Bath: ObjectivesAmit MartinNessuna valutazione finora
- EncephalitisDocumento55 pagineEncephalitisAmit MartinNessuna valutazione finora
- Tuberculin Skin TestDocumento5 pagineTuberculin Skin TestAmit MartinNessuna valutazione finora
- Ultrasound (U.S.G.) : IntroductionDocumento4 pagineUltrasound (U.S.G.) : IntroductionAmit MartinNessuna valutazione finora
- EncephalitisDocumento55 pagineEncephalitisAmit MartinNessuna valutazione finora
- Tuberculin Skin TestDocumento5 pagineTuberculin Skin TestAmit MartinNessuna valutazione finora
- Neurological Pharmacology PresentationDocumento49 pagineNeurological Pharmacology PresentationAmit MartinNessuna valutazione finora
- Nervous System Anatomy and PhysiologyDocumento9 pagineNervous System Anatomy and PhysiologyAmit Martin100% (1)
- Cardiac Examination: / Medication / Mobility AidsDocumento5 pagineCardiac Examination: / Medication / Mobility AidsAmit MartinNessuna valutazione finora
- Type of Shunt For HydrocephalusDocumento3 pagineType of Shunt For HydrocephalusAmit MartinNessuna valutazione finora
- Pharmacological Classification of Drugs First EditionDocumento0 paginePharmacological Classification of Drugs First EditionAmina BećiragićNessuna valutazione finora
- External Otitis (Otitis Externa)Documento16 pagineExternal Otitis (Otitis Externa)Amit MartinNessuna valutazione finora
- Mannitol: Half-Life Onset Peak DurationDocumento3 pagineMannitol: Half-Life Onset Peak DurationAmit MartinNessuna valutazione finora
- CT Scan, Mri, Pet ScanDocumento8 pagineCT Scan, Mri, Pet ScanAmit MartinNessuna valutazione finora
- Anatomy and Physiology of HeartDocumento5 pagineAnatomy and Physiology of HeartAmit MartinNessuna valutazione finora
- CT Scan, Mri, Pet ScanDocumento5 pagineCT Scan, Mri, Pet ScanAmit MartinNessuna valutazione finora
- Vestibular Labyrinthitis: Pathophysiology and EtiologyDocumento3 pagineVestibular Labyrinthitis: Pathophysiology and EtiologyAmit MartinNessuna valutazione finora
- PowerDocumento12 paginePowerAmit MartinNessuna valutazione finora
- Acute Myocardial InfarctionDocumento7 pagineAcute Myocardial InfarctionAmit MartinNessuna valutazione finora
- Cardiovoascular ExamDocumento41 pagineCardiovoascular ExamAmit Martin100% (1)
- Nervous System Anatomy and PhysiologyDocumento9 pagineNervous System Anatomy and PhysiologyAmit Martin100% (1)
- Buddhist Monuments at SanchiDocumento2 pagineBuddhist Monuments at SanchiAmit MartinNessuna valutazione finora
- Range of Motion ExerciseDocumento8 pagineRange of Motion ExerciseAmit Martin83% (6)
- Motor TestingDocumento58 pagineMotor Testingsarguss14100% (2)
- Rhythm SticksDocumento16 pagineRhythm SticksNomer Anthony MadridejoNessuna valutazione finora
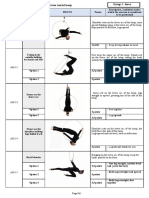
- Appendix 2 Compulsory Exercises Aerial Hoop 2018 EngDocumento28 pagineAppendix 2 Compulsory Exercises Aerial Hoop 2018 Engtito1628100% (1)
- Bujinkan - Ninjutsu - Dojo TermsDocumento17 pagineBujinkan - Ninjutsu - Dojo TermsBinu RadhakrishnanNessuna valutazione finora
- Simple Beginners YogaDocumento49 pagineSimple Beginners YogaShawn CoxNessuna valutazione finora
- Amici PIDocumento353 pagineAmici PIKarl David CalaguiNessuna valutazione finora
- Prashast NCERTDocumento54 paginePrashast NCERTDilip ChakravarthyNessuna valutazione finora
- Computer Masti Book 2Documento116 pagineComputer Masti Book 2rcpuram01Nessuna valutazione finora
- You Are The Universe! (Reiki Self-Healing Treatment)Documento6 pagineYou Are The Universe! (Reiki Self-Healing Treatment)Don Beckett100% (1)
- Growth Predictions / Orthodontic Courses by Indian Dental AcademyDocumento196 pagineGrowth Predictions / Orthodontic Courses by Indian Dental Academyindian dental academy100% (1)
- Bondassage - Kinky EroticDocumento111 pagineBondassage - Kinky EroticJames Stroup100% (1)
- Cara Memakai Handscoon SterilDocumento2 pagineCara Memakai Handscoon Sterilaulia rahmiNessuna valutazione finora
- Biomechanics Labor With Cephalic Presentation ExtensorDocumento2 pagineBiomechanics Labor With Cephalic Presentation ExtensorMed PoxNessuna valutazione finora
- Module 3 Questioned DocumentsDocumento8 pagineModule 3 Questioned DocumentsMid AcidNessuna valutazione finora
- Overload Percussion KeyDocumento2 pagineOverload Percussion KeyLuis Navarrete VelasquezNessuna valutazione finora
- Kriya - Auric Balance and Nerve StrengthDocumento1 paginaKriya - Auric Balance and Nerve StrengthCara CulerNessuna valutazione finora
- HST Catalog Oil GasDocumento9 pagineHST Catalog Oil Gasกัญญารัตน์ พูลทองNessuna valutazione finora
- Epochrypha A Book of Speculative AgesDocumento54 pagineEpochrypha A Book of Speculative AgesPatricia ScrivenerNessuna valutazione finora
- Massage Technique PetrissageDocumento5 pagineMassage Technique PetrissageNelia Banez PatalayNessuna valutazione finora
- Irfan Mir Anatomy Usmle Step 1Documento8 pagineIrfan Mir Anatomy Usmle Step 1sammieahemd100% (1)
- Impact of Nonverbal in International BusinessDocumento25 pagineImpact of Nonverbal in International BusinessHuman Behaviour AcademyNessuna valutazione finora
- Snell Muscle TablesDocumento8 pagineSnell Muscle TablesSmallppNessuna valutazione finora
- Down SyndromeDocumento29 pagineDown SyndromeFatima yasin60% (5)
- Gaya Magnetik GabungDocumento61 pagineGaya Magnetik GabungKurniawan taku lowaNessuna valutazione finora
- Taoist Eight BrocadesDocumento4 pagineTaoist Eight BrocadesfahimNessuna valutazione finora
- Rolando'S Fraciijre OF THE First MetacarpalDocumento2 pagineRolando'S Fraciijre OF THE First MetacarpalVladimir StratanNessuna valutazione finora
- How To Draw Kanji of KujiIn enDocumento24 pagineHow To Draw Kanji of KujiIn enWalter HofmannNessuna valutazione finora
- Growth AssessmentDocumento65 pagineGrowth Assessmentdr parveen bathlaNessuna valutazione finora