Potrebbero piacerti anche
- Psoriasis + StressDocumento8 paginePsoriasis + StressNiatazya Mumtaz SagitaNessuna valutazione finora
- Stress and Periodontal Disease PDFDocumento7 pagineStress and Periodontal Disease PDFDaniela RusnacNessuna valutazione finora
- Psychodermatological Aspects of Atopic DermatitisDocumento6 paginePsychodermatological Aspects of Atopic DermatitisEdu SajquimNessuna valutazione finora
- Orion 2013Documento5 pagineOrion 2013Elaine MedeirosNessuna valutazione finora
- Cohen 2007 Stress and DiseaseDocumento3 pagineCohen 2007 Stress and DiseaseBilly CooperNessuna valutazione finora
- Psychological Stress and Psoriasis: A Systematic Review and Meta-AnalysisDocumento12 paginePsychological Stress and Psoriasis: A Systematic Review and Meta-AnalysisFitrianidilaNessuna valutazione finora
- Acute Multiple Sclerosis RelapseDocumento16 pagineAcute Multiple Sclerosis RelapseHabib G. Moutran BarrosoNessuna valutazione finora
- Stress On ItchDocumento14 pagineStress On Itchdr putriNessuna valutazione finora
- Effects of Stress and Psychological Disorders On The Immune SystemDocumento7 pagineEffects of Stress and Psychological Disorders On The Immune SystemTravis BarkerNessuna valutazione finora
- Psychophysiological Effects of Stress Management in Patients With Atopic Dermatitis: A Randomized Controlled TrialDocumento6 paginePsychophysiological Effects of Stress Management in Patients With Atopic Dermatitis: A Randomized Controlled TrialsnrarasatiNessuna valutazione finora
- Task Resume Article - B InggrisDocumento3 pagineTask Resume Article - B Inggrisalfian khoirun nizamNessuna valutazione finora
- Art:10.1186/s12895 015 0026 XDocumento8 pagineArt:10.1186/s12895 015 0026 XjesikaNessuna valutazione finora
- 1 A 092 F 0382 Bceb 13Documento5 pagine1 A 092 F 0382 Bceb 13kamel abdiNessuna valutazione finora
- Does Stress Increase The Risk of Atopic Dermatitis in Adolescents? Results of The Korea Youth Risk Behavior Web-Based Survey (KYRBWS-VI)Documento10 pagineDoes Stress Increase The Risk of Atopic Dermatitis in Adolescents? Results of The Korea Youth Risk Behavior Web-Based Survey (KYRBWS-VI)Hildy IkhsanNessuna valutazione finora
- Medical Hypotheses 9: 331-335, 1982Documento5 pagineMedical Hypotheses 9: 331-335, 1982Omar DaherNessuna valutazione finora
- Psychosocial Support ofDocumento13 paginePsychosocial Support ofJEFFERSON MUÑOZNessuna valutazione finora
- Ulcera Duodenal y PsicosomtaciaDocumento4 pagineUlcera Duodenal y PsicosomtaciaLuis Fernando Segura LeivaNessuna valutazione finora
- PRD 12036Documento12 paginePRD 12036Rolando Jorge TerrazasNessuna valutazione finora
- AA Bidirectional Relationship Between Psychosocial Factors and Atopic Disorders A Systematic Review and Meta-AnalysisDocumento15 pagineAA Bidirectional Relationship Between Psychosocial Factors and Atopic Disorders A Systematic Review and Meta-AnalysisOlga Rib AsNessuna valutazione finora
- Depression and ObesityDocumento7 pagineDepression and Obesityetherealflames5228Nessuna valutazione finora
- Feb 6 Introd Results Disc GPSY 513 Research Paper References AbstractDocumento6 pagineFeb 6 Introd Results Disc GPSY 513 Research Paper References AbstractEva MartinNessuna valutazione finora
- Department of Dermatology Ospital NG Maynila Medical Center Pamantasan NG Lungsod NG MaynilaDocumento21 pagineDepartment of Dermatology Ospital NG Maynila Medical Center Pamantasan NG Lungsod NG MaynilaAndrean LinataNessuna valutazione finora
- Affective DisordersDocumento37 pagineAffective Disordersveronicaine91Nessuna valutazione finora
- Stressand Autoimmunity: Courtney J. Mccray,, Sandeep K. AgarwalDocumento18 pagineStressand Autoimmunity: Courtney J. Mccray,, Sandeep K. Agarwaltitis dwi tantiNessuna valutazione finora
- Depressive SintomysDocumento6 pagineDepressive SintomysBráulio LimaNessuna valutazione finora
- tmp458B TMPDocumento16 paginetmp458B TMPFrontiersNessuna valutazione finora
- Factores Psicosomaticos en PruritoDocumento10 pagineFactores Psicosomaticos en PruritoMarcos Domic SiedeNessuna valutazione finora
- In Uence of Psychological Stress On Upper Respiratory Infection-A Meta-Analysis of Prospective StudiesDocumento11 pagineIn Uence of Psychological Stress On Upper Respiratory Infection-A Meta-Analysis of Prospective StudiesThang LaNessuna valutazione finora
- Herbal Remedies For Insomnia/anxietyDocumento27 pagineHerbal Remedies For Insomnia/anxietySriram RamamurthyNessuna valutazione finora
- Stress and CopingDocumento7 pagineStress and CopingHrvoje CvitanovicNessuna valutazione finora
- Gelfand 2012Documento5 pagineGelfand 2012gyyygNessuna valutazione finora
- Pathophysiology and Psychodynamics of Disease Causation NewDocumento10 paginePathophysiology and Psychodynamics of Disease Causation NewgemergencycareNessuna valutazione finora
- Jurnal Psiko 6Documento6 pagineJurnal Psiko 6ruryNessuna valutazione finora
- Major Depressive Disorder - New Clinical, Neurobiological, and Treatment PerspectivesDocumento11 pagineMajor Depressive Disorder - New Clinical, Neurobiological, and Treatment PerspectivesArthur KummerNessuna valutazione finora
- Psoriasis and Vascular Disease: An Unsolved Mystery: ReviewDocumento6 paginePsoriasis and Vascular Disease: An Unsolved Mystery: ReviewkendinceNessuna valutazione finora
- Epidemiology: Dr. Siswanto, M.SCDocumento66 pagineEpidemiology: Dr. Siswanto, M.SCArinTa TyArlieNessuna valutazione finora
- tmp33F4 TMPDocumento7 paginetmp33F4 TMPFrontiersNessuna valutazione finora
- Medical News in The World of Atopic Dermatitis First Quarter 2016Documento5 pagineMedical News in The World of Atopic Dermatitis First Quarter 2016anon_384025255Nessuna valutazione finora
- 625Documento8 pagine625thn2u7676Nessuna valutazione finora
- Psoriasis NATURE AYFinlayDocumento48 paginePsoriasis NATURE AYFinlayMelly SyafridaNessuna valutazione finora
- The Role of Inflammation in Depression and Fatigue 2019Documento12 pagineThe Role of Inflammation in Depression and Fatigue 2019Zoltán GöndörNessuna valutazione finora
- Stress Pshycology - B InggrisDocumento4 pagineStress Pshycology - B Inggrisalfian khoirun nizamNessuna valutazione finora
- The Neurobiology of Stress and Gastrointestinal Disease: ReviewDocumento10 pagineThe Neurobiology of Stress and Gastrointestinal Disease: ReviewEstefanía Páez CoyNessuna valutazione finora
- Psycho PsoriasisDocumento61 paginePsycho PsoriasisKhiem Tran DuyNessuna valutazione finora
- How To Cope With PsoriasisDocumento7 pagineHow To Cope With PsoriasisGe NomNessuna valutazione finora
- Important NotesDocumento6 pagineImportant NotesJustabidNessuna valutazione finora
- Burnout Syndrome in Physicians-Psychological Assessment and Biomarker ResearchDocumento11 pagineBurnout Syndrome in Physicians-Psychological Assessment and Biomarker ResearchCarlos Roberto Bautista GuerreroNessuna valutazione finora
- De Ce Ne Imbolnavim (Engleza)Documento9 pagineDe Ce Ne Imbolnavim (Engleza)Ramona BunescuNessuna valutazione finora
- Thesis PsoriasisDocumento4 pagineThesis PsoriasisDereck Downing100% (2)
- 4851-Article Text-14655-2-10-20170116 PDFDocumento14 pagine4851-Article Text-14655-2-10-20170116 PDFKIMNessuna valutazione finora
- 1st LectureDocumento6 pagine1st LectureNoreen FæţįmæNessuna valutazione finora
- Skapinakis Covid 2020Documento11 pagineSkapinakis Covid 2020MicMatzNessuna valutazione finora
- Research Article Depression and Its Relationship With Coping Strategies and Illness Perceptions During The COVID-19 Lockdown in Greece: A Cross-Sectional Survey of The PopulationDocumento11 pagineResearch Article Depression and Its Relationship With Coping Strategies and Illness Perceptions During The COVID-19 Lockdown in Greece: A Cross-Sectional Survey of The PopulationNur FadillaNessuna valutazione finora
- Stress As Bodily ResponseDocumento3 pagineStress As Bodily ResponseRebekah Louise Penrice-RandalNessuna valutazione finora
- Stress and The Periodontium: Review Article 10.5005/jp-Journals-10031-1005Documento3 pagineStress and The Periodontium: Review Article 10.5005/jp-Journals-10031-1005Herpika DianaNessuna valutazione finora
- Impact of Stress On Physical and Mental Health of An IndividualDocumento7 pagineImpact of Stress On Physical and Mental Health of An IndividualNik 19Nessuna valutazione finora
- Mizokami 2004Documento9 pagineMizokami 2004jiadev85Nessuna valutazione finora
- Nstemi + Af RVRDocumento16 pagineNstemi + Af RVRFitrianto Dwi UtomoNessuna valutazione finora
- COVER ForensikDocumento1 paginaCOVER ForensikFitrianto Dwi UtomoNessuna valutazione finora
- Daftar PustakaDocumento2 pagineDaftar PustakaFitrianto Dwi UtomoNessuna valutazione finora
- Case Report: ST Elevation Miocard Infarction AnteroseptalDocumento14 pagineCase Report: ST Elevation Miocard Infarction AnteroseptalFitrianto Dwi UtomoNessuna valutazione finora
- Daftar PustakaDocumento2 pagineDaftar PustakaFitrianto Dwi UtomoNessuna valutazione finora
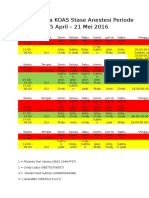
- Jadwal Jaga KOAS Stase Anestesi Periode 25 April - 21 Mei 2016Documento2 pagineJadwal Jaga KOAS Stase Anestesi Periode 25 April - 21 Mei 2016Fitrianto Dwi UtomoNessuna valutazione finora
- CC 9312Documento10 pagineCC 9312Fitrianto Dwi UtomoNessuna valutazione finora
- Daftar Pustak Dr. ArifDocumento4 pagineDaftar Pustak Dr. ArifFitrianto Dwi UtomoNessuna valutazione finora
- Psychophysiological Effects of Stress Management in Patients With Atopic Dermatitis: A Randomized Controlled TrialDocumento6 paginePsychophysiological Effects of Stress Management in Patients With Atopic Dermatitis: A Randomized Controlled TrialsnrarasatiNessuna valutazione finora
- BOOK LIST (Not Complete)Documento12 pagineBOOK LIST (Not Complete)Fitrianto Dwi UtomoNessuna valutazione finora
- Digestive Disease Stats 508 2 PDFDocumento6 pagineDigestive Disease Stats 508 2 PDFFitrianto Dwi UtomoNessuna valutazione finora
- Digestive Disease Stats 508 2 PDFDocumento6 pagineDigestive Disease Stats 508 2 PDFFitrianto Dwi UtomoNessuna valutazione finora
- Gnrs 584 Cduc Mphi Dap Presentation Schizoaffective DisorderDocumento17 pagineGnrs 584 Cduc Mphi Dap Presentation Schizoaffective Disorderapi-437250138Nessuna valutazione finora
- Objective Personality Assessment Class 8Documento87 pagineObjective Personality Assessment Class 8lpiechphdNessuna valutazione finora
- 2020 Eating DisordersDocumento13 pagine2020 Eating DisordersNathália CristimannNessuna valutazione finora
- AnxietyDocumento4 pagineAnxietyAnn DassNessuna valutazione finora
- Attention Deficit Hyperactivity DisorderDocumento10 pagineAttention Deficit Hyperactivity Disorderapi-3797941100% (1)
- Diseases Written by Harriet Bailey in 1920 and The First Psychiatric Nursing TheoristDocumento2 pagineDiseases Written by Harriet Bailey in 1920 and The First Psychiatric Nursing TheoristNaifah AbdullahNessuna valutazione finora
- GENERALIZED ANXIETY DISORDER (Script)Documento3 pagineGENERALIZED ANXIETY DISORDER (Script)Kian Justin HidalgoNessuna valutazione finora
- Hoarding DisorderDocumento22 pagineHoarding Disorderrumela.kunduNessuna valutazione finora
- Research LiteratureDocumento1 paginaResearch LiteratureThe Seafarer RamNessuna valutazione finora
- Material On Theme of Adolescent Problem - Amrutha S - 1st B.ed EnglishDocumento26 pagineMaterial On Theme of Adolescent Problem - Amrutha S - 1st B.ed EnglishAmruthaNessuna valutazione finora
- 1.3.+delusions+ +hallucinations-1Documento24 pagine1.3.+delusions+ +hallucinations-1Anonymous sSR6x6VC8aNessuna valutazione finora
- Essay - Adhd RSDDocumento12 pagineEssay - Adhd RSDapi-549234312Nessuna valutazione finora
- ScriptDocumento1 paginaScriptSherlyn Miranda GarcesNessuna valutazione finora
- Mental Status Examination - StatPearls - NCBI BookshelfDocumento9 pagineMental Status Examination - StatPearls - NCBI BookshelfGRUPO DE INTERES EN PSIQUIATRIANessuna valutazione finora
- PPPD HandoutDocumento3 paginePPPD HandoutBryanNessuna valutazione finora
- Rosewood Centers For Eating Disorders Strengthens Offerings With Co-Occurring Disorders CareDocumento3 pagineRosewood Centers For Eating Disorders Strengthens Offerings With Co-Occurring Disorders CarePR.comNessuna valutazione finora
- Hronis Et Al. (2019) Fearless Me!© - A Feasibility Case Series of Cognitive Behavioral Therapy For Adolescents With Intellectual DisabilityDocumento15 pagineHronis Et Al. (2019) Fearless Me!© - A Feasibility Case Series of Cognitive Behavioral Therapy For Adolescents With Intellectual DisabilityPhilip BeardNessuna valutazione finora
- Psychopaths 2Documento23 paginePsychopaths 2api-283565717100% (1)
- D.I.D BrochureDocumento1 paginaD.I.D Brochurehbanafsh2119Nessuna valutazione finora
- Risk For Acute Confusion 1-4Documento2 pagineRisk For Acute Confusion 1-4DewiRestiNazullyQiran100% (1)
- Psychological Analysis of Girl InterruptedDocumento2 paginePsychological Analysis of Girl InterruptedGeorge Baywong100% (1)
- QuestionDocumento8 pagineQuestionBire Rohidas SureshNessuna valutazione finora
- Handbook of Chronic Depression Diagnosis and Therapeutic Management Medical Psychiatry 25Documento470 pagineHandbook of Chronic Depression Diagnosis and Therapeutic Management Medical Psychiatry 25Milos100% (1)
- EZCare Clinic Now Offers ADD or ADHD Treatment. Diagnostic Exam For New Patients and Prescription Refills Available Today.Documento3 pagineEZCare Clinic Now Offers ADD or ADHD Treatment. Diagnostic Exam For New Patients and Prescription Refills Available Today.PR.comNessuna valutazione finora
- BorderlineDocumento12 pagineBorderlineksqvrkz4dmNessuna valutazione finora
- H-Unit 05-B.Pharmacy 4th Semester - Pharamcology.Documento3 pagineH-Unit 05-B.Pharmacy 4th Semester - Pharamcology.raviomj100% (1)
- Could It Be ADHD - ADHD Self Assessment Workbook (The Mini ADHD Coach)Documento61 pagineCould It Be ADHD - ADHD Self Assessment Workbook (The Mini ADHD Coach)andres mena100% (1)
- DSM Iv TRDocumento5 pagineDSM Iv TRTri Bunda AqshoNessuna valutazione finora
- Dyslexia and Specific Learning Disorders New International Diagnostic CriteriaDocumento6 pagineDyslexia and Specific Learning Disorders New International Diagnostic CriteriaTimothy Eduard A. SupitNessuna valutazione finora
- Child Adolescent Psychological EvaluationDocumento38 pagineChild Adolescent Psychological EvaluationdrrajivmohtaNessuna valutazione finora