Potrebbero piacerti anche
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (895)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (344)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (121)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (74)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- 100 Postcolonial SGDocumento61 pagine100 Postcolonial SGAmalAhmedKamal100% (1)
- Hubungan Pengetahuan Dengan Sikap: Case Processing SummaryDocumento17 pagineHubungan Pengetahuan Dengan Sikap: Case Processing SummaryRatnaWFebryNessuna valutazione finora
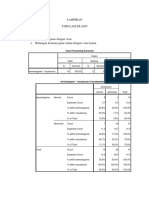
- Lampiran Tabulasi Silang: Case Processing SummaryDocumento13 pagineLampiran Tabulasi Silang: Case Processing SummaryRatnaWFebryNessuna valutazione finora
- PathwayDocumento1 paginaPathwayRatnaWFebryNessuna valutazione finora
- Effect of Anxiety Disorder On Impairment and Recovery From StrokeDocumento7 pagineEffect of Anxiety Disorder On Impairment and Recovery From StrokeRatnaWFebryNessuna valutazione finora
- Diabetes MelitusDocumento6 pagineDiabetes MelitusRatnaWFebryNessuna valutazione finora
- Erotic CultDocumento6 pagineErotic Cultmallikai_1Nessuna valutazione finora
- What Is Dark Energy?Documento20 pagineWhat Is Dark Energy?Harsh DhyaniNessuna valutazione finora
- Art Intg Proj CL 6-10Documento5 pagineArt Intg Proj CL 6-10Sarthak JoshiNessuna valutazione finora
- NotesDocumento33 pagineNotesMohammad ZaheerNessuna valutazione finora
- Bit Sub and Float ChartDocumento16 pagineBit Sub and Float ChartRobert KilgoreNessuna valutazione finora
- Arlene Dickinson, All inDocumento2 pagineArlene Dickinson, All inkinayath@yahoo.comNessuna valutazione finora
- Reviewer in Campus JournalismDocumento49 pagineReviewer in Campus JournalismJennifer L. Magboo-OestarNessuna valutazione finora
- P. Cartier, D. Foata (Auth.) - Problèmes Combinatoires de Commutation Et RéarrangementsDocumento81 pagineP. Cartier, D. Foata (Auth.) - Problèmes Combinatoires de Commutation Et RéarrangementsDJEHA14Nessuna valutazione finora
- KABIR HASION CV Executive-1 PDFDocumento2 pagineKABIR HASION CV Executive-1 PDFraiyanduNessuna valutazione finora
- Annotated BibliographyDocumento17 pagineAnnotated Bibliographyapi-2531405230% (1)
- RHDHV Nereda EN PDFDocumento8 pagineRHDHV Nereda EN PDFdmnNessuna valutazione finora
- Manual de Usuario 4010ESDocumento1 paginaManual de Usuario 4010ESRobel MTNessuna valutazione finora
- Paraphrasing ExercisesDocumento4 pagineParaphrasing ExercisesPaulinaNessuna valutazione finora
- SREHD Article in Army Alt April-June-2017Documento5 pagineSREHD Article in Army Alt April-June-2017dvtherionNessuna valutazione finora
- E3 - Identify Purpose of Components and Build CircuitsDocumento2 pagineE3 - Identify Purpose of Components and Build Circuitsapi-316704749Nessuna valutazione finora
- OdorizationDocumento5 pagineOdorizationShreya Sahajpal KaushalNessuna valutazione finora
- The Historical & Evolutionary Theory of The Origin of StateDocumento5 pagineThe Historical & Evolutionary Theory of The Origin of StateMateen Ali100% (1)
- BIM Project Execution Planning Guide and Templates - V2.1Documento1 paginaBIM Project Execution Planning Guide and Templates - V2.1NajaAlwi100% (1)
- Adt 11-1Documento27 pagineAdt 11-1Paul Bustamante BermalNessuna valutazione finora
- Testing MechanicalDocumento42 pagineTesting MechanicalSadique ChakoleNessuna valutazione finora
- An Understanding of Psychometric ToolsDocumento4 pagineAn Understanding of Psychometric ToolsAntariksh Bhandari100% (1)
- Art EducationDocumento13 pagineArt EducationJaime MorrisNessuna valutazione finora
- Primavera P6Documento2 paginePrimavera P6tutan12000Nessuna valutazione finora
- 2023 Occ 1ST ExamDocumento3 pagine2023 Occ 1ST ExamSamantha LaboNessuna valutazione finora
- Rooms Division DepartmentDocumento7 pagineRooms Division Departmentlil_jinkz09Nessuna valutazione finora
- Perception of Coc Pup Students For Twitter As A Source of InformationDocumento28 paginePerception of Coc Pup Students For Twitter As A Source of Informationmark aljon fajardoNessuna valutazione finora
- How To Live To Be 200Documento3 pagineHow To Live To Be 200Anonymous 117cflkW9W100% (2)
- Multiple Routes Routing in Computer Networks Remote DistanceDocumento3 pagineMultiple Routes Routing in Computer Networks Remote DistanceerpublicationNessuna valutazione finora
- Gestalt Peeling The Onion Csi Presentatin March 12 2011Documento6 pagineGestalt Peeling The Onion Csi Presentatin March 12 2011Adriana Bogdanovska ToskicNessuna valutazione finora