Potrebbero piacerti anche
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (121)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (588)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (400)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (266)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5795)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (345)
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (895)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- Physical Education SBA G.GajieDocumento29 paginePhysical Education SBA G.Gajieselina fraser83% (6)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- Collarbone Breathing TreatmentDocumento4 pagineCollarbone Breathing TreatmentPatrizioNessuna valutazione finora
- Clinical Evaluation FormDocumento1 paginaClinical Evaluation FormAndalNessuna valutazione finora
- Antidepressants AntidepressantsDocumento38 pagineAntidepressants AntidepressantsjaneNessuna valutazione finora
- Types of Therapeutic DietsDocumento10 pagineTypes of Therapeutic DietsFaith Marfil100% (1)
- Ap Lang Memoir EssayDocumento13 pagineAp Lang Memoir Essayapi-305343417100% (1)
- GTD Case StudyDocumento9 pagineGTD Case StudyZnarf Izlah Sadanreb100% (1)
- Etiology of Tuberculosis PDFDocumento2 pagineEtiology of Tuberculosis PDFKevinNessuna valutazione finora
- Final Osce Care PlanDocumento8 pagineFinal Osce Care Planapi-526590140100% (1)
- NIH Public Access: Delayed Antimicrobial Therapy Increases Mortality and Organ Dysfunction Duration in Pediatric SepsisDocumento23 pagineNIH Public Access: Delayed Antimicrobial Therapy Increases Mortality and Organ Dysfunction Duration in Pediatric SepsisjaneNessuna valutazione finora
- Radiology Icm IiDocumento8 pagineRadiology Icm IijaneNessuna valutazione finora
- Intratympanic Membrane Congenital CholesteatomaDocumento3 pagineIntratympanic Membrane Congenital CholesteatomajaneNessuna valutazione finora
- Medical Leadership Competency Framework: Landscape of HealthcareDocumento15 pagineMedical Leadership Competency Framework: Landscape of HealthcarejaneNessuna valutazione finora
- By: Dr. Engelberta Sp. KJDocumento14 pagineBy: Dr. Engelberta Sp. KJjaneNessuna valutazione finora
- Substance Abuse Among Health Professionals: August 15, 2014Documento25 pagineSubstance Abuse Among Health Professionals: August 15, 2014janeNessuna valutazione finora
- Transient Loss of Consciousness: History TakingDocumento4 pagineTransient Loss of Consciousness: History TakingjaneNessuna valutazione finora
- Itching, Redness of The SkinDocumento21 pagineItching, Redness of The SkinjaneNessuna valutazione finora
- Lymphokines & Cytokines: Immunology & DiseaseDocumento34 pagineLymphokines & Cytokines: Immunology & DiseasejaneNessuna valutazione finora
- To Physiology, Homeostasis, and Body Temperature: V. Sutarmo SetiadjiDocumento20 pagineTo Physiology, Homeostasis, and Body Temperature: V. Sutarmo SetiadjijaneNessuna valutazione finora
- Mechanisms of Antibiotic Resistance in BacteriaDocumento40 pagineMechanisms of Antibiotic Resistance in BacteriajaneNessuna valutazione finora
- Mechanisms of Antibiotic Resistance in BacteriaDocumento41 pagineMechanisms of Antibiotic Resistance in BacteriajaneNessuna valutazione finora
- JawsDocumento78 pagineJawsjaneNessuna valutazione finora
- COMMUNICATION With Other ProfessionalsDocumento12 pagineCOMMUNICATION With Other ProfessionalsjaneNessuna valutazione finora
- STM Cels Lcture 1Documento44 pagineSTM Cels Lcture 1janeNessuna valutazione finora
- LibraryDocumento1 paginaLibraryjaneNessuna valutazione finora
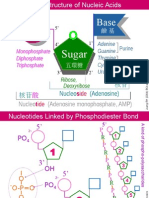
- NA01 StructureDocumento5 pagineNA01 StructurejaneNessuna valutazione finora
- Resume 2 SampleDocumento3 pagineResume 2 SampleDominique Lim YañezNessuna valutazione finora
- Home-Made HBsAgDocumento1 paginaHome-Made HBsAgsomchaisNessuna valutazione finora
- Disease and Disease TransmissionDocumento48 pagineDisease and Disease TransmissionAYO NELSONNessuna valutazione finora
- A Pharmacology-Based Comprehensive Review On Medicinal PlantsDocumento14 pagineA Pharmacology-Based Comprehensive Review On Medicinal PlantsissamebenNessuna valutazione finora
- Prognostic Factors Affecting The Mortality of Burn Injuries Patients in Dr. Sardjito General Hospital, Yogyakarta, IndonesiaDocumento8 paginePrognostic Factors Affecting The Mortality of Burn Injuries Patients in Dr. Sardjito General Hospital, Yogyakarta, IndonesiaYeni PuspitasariNessuna valutazione finora
- Strategies For Acute Metabolic DisordersDocumento14 pagineStrategies For Acute Metabolic DisordersAhmed AnwarNessuna valutazione finora
- Others Districts Others Districts Others Districts Others DistrictsDocumento6 pagineOthers Districts Others Districts Others Districts Others DistrictsThulasiraman AshokkumarNessuna valutazione finora
- The Benefits of Immunotherapy CombinationsDocumento1 paginaThe Benefits of Immunotherapy CombinationsMicheleFontanaNessuna valutazione finora
- Indices MeasuringDocumento27 pagineIndices Measuringdinesh11rNessuna valutazione finora
- Antibiotic Prophylaxis in Dentistry: A Review and Practice RecommendationsDocumento9 pagineAntibiotic Prophylaxis in Dentistry: A Review and Practice RecommendationsDina AnisawatiNessuna valutazione finora
- DietitianDocumento2 pagineDietitianapi-121434245Nessuna valutazione finora
- Practical Guide To Insulin Therapy in Type 2 Diabetes: January 2011Documento91 paginePractical Guide To Insulin Therapy in Type 2 Diabetes: January 2011leeyie22Nessuna valutazione finora
- Evaluation of The Nutritional Supplement VIUSID Vet Powder On The Productive Behaviour of Sows and BoarsDocumento8 pagineEvaluation of The Nutritional Supplement VIUSID Vet Powder On The Productive Behaviour of Sows and BoarsAgnes TamrinNessuna valutazione finora
- Teaching-Plan-Health-Education-Plan-Diabetes Mellitus TYPE IIDocumento3 pagineTeaching-Plan-Health-Education-Plan-Diabetes Mellitus TYPE IIkasjdkasNessuna valutazione finora
- S Curvy .: Lobna Hani HijliDocumento4 pagineS Curvy .: Lobna Hani Hijlilobna HijliNessuna valutazione finora
- Clinical Approach To A Patient With Dysphagia: Medicine UpdateDocumento3 pagineClinical Approach To A Patient With Dysphagia: Medicine UpdateAnonymous XFDJfsGviNessuna valutazione finora
- General AnesthesiaDocumento22 pagineGeneral AnesthesiaDr Anais AsimNessuna valutazione finora
- CN 9-12Documento6 pagineCN 9-12The Real UploaderNessuna valutazione finora
- Anggraini & Pusspasari 2019Documento8 pagineAnggraini & Pusspasari 2019Berlianti Citra MaulidyaNessuna valutazione finora
- Naskah BING4434 The 1Documento3 pagineNaskah BING4434 The 1Jesslin SparklingNessuna valutazione finora
- Virani Et Al 2021 Heart Disease and Stroke Statistics 2021 UpdateDocumento490 pagineVirani Et Al 2021 Heart Disease and Stroke Statistics 2021 UpdatehendridunantikoNessuna valutazione finora
- Mock Ospe Me211Documento15 pagineMock Ospe Me211sahirbuleNessuna valutazione finora