Potrebbero piacerti anche
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- SSM-11th Edn Full IndexDocumento62 pagineSSM-11th Edn Full Indexece142Nessuna valutazione finora
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5795)
- Pharma Corner - Sample Study MaterilasDocumento17 paginePharma Corner - Sample Study MaterilasAmit PatelNessuna valutazione finora
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (895)
- 2017-05-01 Final Nystatin Notice To Customer Letter PDFDocumento2 pagine2017-05-01 Final Nystatin Notice To Customer Letter PDFsaidvaretNessuna valutazione finora
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- List of Substandard Drugs2005Documento7 pagineList of Substandard Drugs2005Mohammad Shahbaz AlamNessuna valutazione finora
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (588)
- Asperheim Introduction To PharmacologyDocumento308 pagineAsperheim Introduction To PharmacologyhsxvskgtrhNessuna valutazione finora
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (400)
- Association of SGLT2 Inhibitors With Arrhythmias and Sudden Cardiac Death Meta-AnalysisDocumento8 pagineAssociation of SGLT2 Inhibitors With Arrhythmias and Sudden Cardiac Death Meta-AnalysisMacarenaNessuna valutazione finora
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- Practical Psychopharmacology in Children and Adolescents: Anoop Vermani MD Fellow, Child and Adolescent PsychiatryDocumento29 paginePractical Psychopharmacology in Children and Adolescents: Anoop Vermani MD Fellow, Child and Adolescent PsychiatryShahinaz ShamsNessuna valutazione finora
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- MTP 170513153856Documento43 pagineMTP 170513153856Sachin SinghNessuna valutazione finora
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2259)
- Pharmacological Properties of Podophyllum Hexandrum Royle: A Comprehensive ReviewDocumento12 paginePharmacological Properties of Podophyllum Hexandrum Royle: A Comprehensive ReviewIJAR JOURNALNessuna valutazione finora
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (74)
- A Systematic Review of Complex Polypharmacy in Bipolar DisorderDocumento12 pagineA Systematic Review of Complex Polypharmacy in Bipolar DisorderalejandraNessuna valutazione finora
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
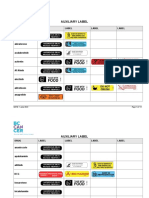
- Auxiliary Label LISTDocumento14 pagineAuxiliary Label LISTAbdur RachmanNessuna valutazione finora
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- Lexicomp® Drug Interactions - UpToDateDocumento2 pagineLexicomp® Drug Interactions - UpToDateDiana PhamNessuna valutazione finora
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- New Methodology For The N-Demethylation of Opiate Alkaloids: Zemin Dong and Peter J. ScammellsDocumento5 pagineNew Methodology For The N-Demethylation of Opiate Alkaloids: Zemin Dong and Peter J. ScammellsJohn PerryNessuna valutazione finora
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (266)
- 2022 HRS - Aggressive B-Cell Lymphomas FINALDocumento80 pagine2022 HRS - Aggressive B-Cell Lymphomas FINALИван НегарэNessuna valutazione finora
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (345)
- Hoarding SyndromeDocumento55 pagineHoarding SyndromeIrish Eunice FelixNessuna valutazione finora
- MetoprololDocumento15 pagineMetoprololMahavir SinghNessuna valutazione finora
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- Nicotine - It May Have A Good Side - Harvard HealthDocumento3 pagineNicotine - It May Have A Good Side - Harvard HealthzimkoNessuna valutazione finora
- ANTI Cancer DrugDocumento11 pagineANTI Cancer DrugAmina AmiarNessuna valutazione finora
- Toxicological Effects of Camellia Sinensis Green Tea A Review-With-Cover-Page-V2Documento9 pagineToxicological Effects of Camellia Sinensis Green Tea A Review-With-Cover-Page-V2KalilNessuna valutazione finora
- IndaloptreDocumento8 pagineIndaloptreTushar PunjaniNessuna valutazione finora
- Antibiotic GuidelineDocumento11 pagineAntibiotic GuidelineSanjay ShresthaNessuna valutazione finora
- Pharmaceutical Sciences: Pharmacy PrepDocumento238 paginePharmaceutical Sciences: Pharmacy Prepabob619100% (1)
- Iorizzo2015 PDFDocumento9 pagineIorizzo2015 PDFEka SyahriniNessuna valutazione finora
- Abnormal Sexuality and Sexual DysfunctionsDocumento8 pagineAbnormal Sexuality and Sexual DysfunctionsIsabel CastilloNessuna valutazione finora
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- Nifedipine Drug StudyDocumento3 pagineNifedipine Drug StudyCrystal Queen MarquezNessuna valutazione finora
- Anacardium Occidentale 5Documento7 pagineAnacardium Occidentale 5Jesus Llorente MendozaNessuna valutazione finora
- Chapter 1 PPT 2 (Container and Closures)Documento15 pagineChapter 1 PPT 2 (Container and Closures)Shumaila Qadir100% (2)
- Hydroxyetyl StarchDocumento10 pagineHydroxyetyl StarchKarina RosamelcachoNessuna valutazione finora
- Adrenergic NeurotransmittersDocumento18 pagineAdrenergic Neurotransmittersparmarkeval1610Nessuna valutazione finora
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (121)
- Research Chap 1 3Documento46 pagineResearch Chap 1 3Skyla FiestaNessuna valutazione finora
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)