Potrebbero piacerti anche
- 09 - Monitoring and Complications of Parenteral NutritionDocumento14 pagine09 - Monitoring and Complications of Parenteral Nutritionbocah_britpopNessuna valutazione finora
- 17 - Enhanced Recovery PrinciplesDocumento7 pagine17 - Enhanced Recovery Principlesbocah_britpopNessuna valutazione finora
- 08 - Oral and Sip FeedingDocumento11 pagine08 - Oral and Sip Feedingbocah_britpopNessuna valutazione finora
- Interaction of Bone and Vascular Disease in CKDDocumento7 pagineInteraction of Bone and Vascular Disease in CKDbocah_britpopNessuna valutazione finora
- 03 - Nutritional Screening and Assessment PDFDocumento8 pagine03 - Nutritional Screening and Assessment PDFbocah_britpop100% (1)
- 17 - Enhanced Recovery PrinciplesDocumento7 pagine17 - Enhanced Recovery Principlesbocah_britpopNessuna valutazione finora
- Materi PerioperatifDocumento11 pagineMateri PerioperatifSyahdat NurkholiqNessuna valutazione finora
- 17 - The Traumatized PatientDocumento7 pagine17 - The Traumatized Patientbocah_britpopNessuna valutazione finora
- 03 - Energy BalanceDocumento8 pagine03 - Energy Balancebocah_britpopNessuna valutazione finora
- 17 - Enhanced Recovery PrinciplesDocumento7 pagine17 - Enhanced Recovery Principlesbocah_britpopNessuna valutazione finora
- 17 - The Traumatized PatientDocumento7 pagine17 - The Traumatized Patientbocah_britpopNessuna valutazione finora
- 09 - Compounding and Ready-To-use Preparation of PN Pharmaceutical Aspects. Compatibility and Stability Consideration DrugDocumento21 pagine09 - Compounding and Ready-To-use Preparation of PN Pharmaceutical Aspects. Compatibility and Stability Consideration Drugbocah_britpopNessuna valutazione finora
- m84 PDFDocumento14 paginem84 PDFMico Ga Bisa GendutNessuna valutazione finora
- 08 - Complications and Monitoring of enDocumento7 pagine08 - Complications and Monitoring of enbocah_britpopNessuna valutazione finora
- 08 - Techniques of Enteral NutritionDocumento16 pagine08 - Techniques of Enteral Nutritionbocah_britpopNessuna valutazione finora
- 08 - Oral and Sip FeedingDocumento11 pagine08 - Oral and Sip Feedingbocah_britpopNessuna valutazione finora
- Materi PerioperatifDocumento11 pagineMateri PerioperatifSyahdat NurkholiqNessuna valutazione finora
- Indications, Contraindications and Monitoring of Enteral NutritionDocumento13 pagineIndications, Contraindications and Monitoring of Enteral Nutritionbocah_britpopNessuna valutazione finora
- Presentation 1Documento2 paginePresentation 1bocah_britpopNessuna valutazione finora
- Weekly ChartDocumento7 pagineWeekly Chartbocah_britpopNessuna valutazione finora
- IAH ACS Medical Management 2014Documento1 paginaIAH ACS Medical Management 2014bocah_britpopNessuna valutazione finora
- ACS SabistonDocumento10 pagineACS Sabistonbocah_britpopNessuna valutazione finora
- Upper Abdominal Pain Case ReportDocumento2 pagineUpper Abdominal Pain Case Reportbocah_britpopNessuna valutazione finora
- Interaction of Bone and Vascular Disease in CKDDocumento7 pagineInteraction of Bone and Vascular Disease in CKDbocah_britpopNessuna valutazione finora
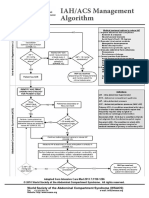
- IAH/ACS Management Algorithm Adapted from Intensive Care MedDocumento1 paginaIAH/ACS Management Algorithm Adapted from Intensive Care Medbocah_britpopNessuna valutazione finora
- HydrocephalusDocumento51 pagineHydrocephalusbocah_britpopNessuna valutazione finora
- Intraabdominal Pressure MonitoringDocumento10 pagineIntraabdominal Pressure Monitoringbocah_britpopNessuna valutazione finora
- Case Disc RadioDocumento29 pagineCase Disc Radiobocah_britpopNessuna valutazione finora
- University of Colorado NICHE Practice Survey SummaryDocumento48 pagineUniversity of Colorado NICHE Practice Survey Summarybocah_britpopNessuna valutazione finora
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (894)
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (265)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (73)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (119)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- Rtlo 18918B 1202Documento42 pagineRtlo 18918B 1202gustavomosqueraalbornozNessuna valutazione finora
- Request For AffidavitDocumento2 pagineRequest For AffidavitGhee MoralesNessuna valutazione finora
- Personal InsuranceDocumento11 paginePersonal InsuranceSumit Kumar SharmaNessuna valutazione finora
- Kunci Jawaban Creative English 3BDocumento14 pagineKunci Jawaban Creative English 3BLedjab Fatima67% (3)
- Easyjet Group6Documento11 pagineEasyjet Group6Rishabh RakhechaNessuna valutazione finora
- NH School Employee Criminal Record Check FormDocumento2 pagineNH School Employee Criminal Record Check FormEmily LescatreNessuna valutazione finora
- BCM Risk Management and Compliance Training in JakartaDocumento2 pagineBCM Risk Management and Compliance Training in Jakartaindra gNessuna valutazione finora
- Company's Profile Presentation (Mauritius Commercial Bank)Documento23 pagineCompany's Profile Presentation (Mauritius Commercial Bank)ashairways100% (2)
- Courier - Capstone WebApp - Round 3 ReportDocumento23 pagineCourier - Capstone WebApp - Round 3 Reportmarmounette26Nessuna valutazione finora
- FZ16 9B 1KD2 (Patada) PDFDocumento62 pagineFZ16 9B 1KD2 (Patada) PDFPanthukalathil Ram100% (1)
- The Non Technical Part: Sample Interview Questions For Network EngineersDocumento5 pagineThe Non Technical Part: Sample Interview Questions For Network EngineersblablaNessuna valutazione finora
- Schedule of Charges General Banking 2022Documento18 pagineSchedule of Charges General Banking 2022Shohag MahmudNessuna valutazione finora
- Fleck 3150 Downflow: Service ManualDocumento40 pagineFleck 3150 Downflow: Service ManualLund2016Nessuna valutazione finora
- Namal College Admissions FAQsDocumento3 pagineNamal College Admissions FAQsSauban AhmedNessuna valutazione finora
- De Thi Thu THPT Quoc Gia Mon Tieng Anh Truong THPT Hai An Hai Phong Nam 2015Documento10 pagineDe Thi Thu THPT Quoc Gia Mon Tieng Anh Truong THPT Hai An Hai Phong Nam 2015nguyen ngaNessuna valutazione finora
- Letter of Recommendation For Nicolas Hallett From Big Ten Network's Casey Peterson.Documento1 paginaLetter of Recommendation For Nicolas Hallett From Big Ten Network's Casey Peterson.Nic HallettNessuna valutazione finora
- Perbandingan Sistem Pemerintahan Dalam Hal Pemilihan Kepala Negara Di Indonesia Dan SingapuraDocumento9 paginePerbandingan Sistem Pemerintahan Dalam Hal Pemilihan Kepala Negara Di Indonesia Dan SingapuraRendy SuryaNessuna valutazione finora
- Marketing Management NotesDocumento115 pagineMarketing Management NotesKajwangs DanNessuna valutazione finora
- Risk Ology ManualDocumento2 pagineRisk Ology ManualGregoryNessuna valutazione finora
- Fact Sheet Rocket StovesDocumento2 pagineFact Sheet Rocket StovesMorana100% (1)
- James Ashmore - Curriculum VitaeDocumento2 pagineJames Ashmore - Curriculum VitaeJames AshmoreNessuna valutazione finora
- SHIPPING TERMSDocumento1 paginaSHIPPING TERMSGung Mayura100% (1)
- Intermediate Accounting Testbank 2Documento419 pagineIntermediate Accounting Testbank 2SOPHIA97% (30)
- Safety of High-Rise BuildingsDocumento14 pagineSafety of High-Rise BuildingsHananeel Sandhi100% (2)
- Chi Square LessonDocumento11 pagineChi Square LessonKaia HamadaNessuna valutazione finora
- MMPX 403 Parametr ListDocumento30 pagineMMPX 403 Parametr ListOğuz Kağan ÖkdemNessuna valutazione finora
- UBI1Documento66 pagineUBI1Rudra SinghNessuna valutazione finora
- 34 Annual Report 2019 20Documento238 pagine34 Annual Report 2019 20Rahul N PatelNessuna valutazione finora
- Numark MixTrack Pro II Traktor ProDocumento3 pagineNumark MixTrack Pro II Traktor ProSantiCai100% (1)
- MT R 108 000 0 000000-0 DHHS B eDocumento68 pagineMT R 108 000 0 000000-0 DHHS B eRafal WojciechowskiNessuna valutazione finora