Potrebbero piacerti anche
- Preanesthetic Evaluation in Private Practice: Richard M.M. Flowerdew, MB, BS, FRCA (London, England)Documento13 paginePreanesthetic Evaluation in Private Practice: Richard M.M. Flowerdew, MB, BS, FRCA (London, England)PaulShaneHerreraZorrillaNessuna valutazione finora
- Preg Hypertension Guidelines PDFDocumento41 paginePreg Hypertension Guidelines PDFPaulShaneHerreraZorrillaNessuna valutazione finora
- From The Laboratories of The Rockefeller Institute/or Medical ResearchDocumento40 pagineFrom The Laboratories of The Rockefeller Institute/or Medical ResearchPaulShaneHerreraZorrillaNessuna valutazione finora
- 5 Cardiac Risk of NonDocumento14 pagine5 Cardiac Risk of NonPaulShaneHerreraZorrillaNessuna valutazione finora
- Tranexamic Acid in Trauma. ¿How Should We Use It (2013)Documento12 pagineTranexamic Acid in Trauma. ¿How Should We Use It (2013)Enzo_AENessuna valutazione finora
- 02 Bfe 510016773 Ea 7 D 000000Documento11 pagine02 Bfe 510016773 Ea 7 D 000000PaulShaneHerreraZorrillaNessuna valutazione finora
- 1 s2.0 S0034935614700155 MainDocumento25 pagine1 s2.0 S0034935614700155 MainPaulShaneHerreraZorrillaNessuna valutazione finora
- Maegele 2016 TransfusionDocumento9 pagineMaegele 2016 TransfusionPaulShaneHerreraZorrillaNessuna valutazione finora
- Slow and LowDocumento21 pagineSlow and LowPaulShaneHerreraZorrillaNessuna valutazione finora
- Surgical Apgar Score Applicability in Patients Undergoing Laparatomy at Kenyatta National HospitalDocumento49 pagineSurgical Apgar Score Applicability in Patients Undergoing Laparatomy at Kenyatta National HospitalPaulShaneHerreraZorrillaNessuna valutazione finora
- CG00081 Fluid MX Revised April 2016Documento11 pagineCG00081 Fluid MX Revised April 2016PaulShaneHerreraZorrillaNessuna valutazione finora
- AnApgarScoreforSurgery PDFDocumento8 pagineAnApgarScoreforSurgery PDFPaulShaneHerreraZorrillaNessuna valutazione finora
- Blood Based ResuscitationDocumento25 pagineBlood Based ResuscitationPaulShaneHerreraZorrillaNessuna valutazione finora
- X Artikel Damage Control TraumaDocumento8 pagineX Artikel Damage Control TraumaPaulShaneHerreraZorrillaNessuna valutazione finora
- Holley Transfusion and Coagulopathy 130902114337 Phpapp01Documento71 pagineHolley Transfusion and Coagulopathy 130902114337 Phpapp01PaulShaneHerreraZorrillaNessuna valutazione finora
- NYSORA Lower ExtremityDocumento1 paginaNYSORA Lower ExtremityPaulShaneHerreraZorrillaNessuna valutazione finora
- Resuscitation and Transfusion Management in Trauma Patients - Emerging Co - SFLBDocumento10 pagineResuscitation and Transfusion Management in Trauma Patients - Emerging Co - SFLBPaulShaneHerreraZorrillaNessuna valutazione finora
- Kwan Et Al-2014-The Cochrane LibraryDocumento20 pagineKwan Et Al-2014-The Cochrane LibraryPaulShaneHerreraZorrillaNessuna valutazione finora
- Damage Control ResuscitationDocumento24 pagineDamage Control ResuscitationPaulShaneHerreraZorrillaNessuna valutazione finora
- 01 - Cook - Damage Control Resuscitation 2Documento50 pagine01 - Cook - Damage Control Resuscitation 2PaulShaneHerreraZorrillaNessuna valutazione finora
- AnesDocumento8 pagineAnesErani SukmaNessuna valutazione finora
- 3WiseMen PermissiveHypotension BeebeDocumento6 pagine3WiseMen PermissiveHypotension BeebePaulShaneHerreraZorrillaNessuna valutazione finora
- Blood Pressure RegulationDocumento11 pagineBlood Pressure RegulationPaulShaneHerreraZorrillaNessuna valutazione finora
- CardiovascDocumento8 pagineCardiovasc21250972Nessuna valutazione finora
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (400)
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (588)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (74)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (266)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (344)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (121)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- Qing 2019Documento9 pagineQing 2019santi lestariNessuna valutazione finora
- Articulo Farmacologia PDFDocumento4 pagineArticulo Farmacologia PDFMichelle RojoNessuna valutazione finora
- Chronic MegacolonDocumento3 pagineChronic Megacolondrnareshkumar3281Nessuna valutazione finora
- Bone BiopsyDocumento3 pagineBone BiopsySophia A. GoNessuna valutazione finora
- Maklumat Vaksinasi: Vaccination DetailsDocumento2 pagineMaklumat Vaksinasi: Vaccination DetailsNORFADHLI ARIFNessuna valutazione finora
- Pediatric Medication AdministrationDocumento59 paginePediatric Medication AdministrationHilary Alvarado100% (1)
- Mock Congress Bill Research EssayDocumento9 pagineMock Congress Bill Research Essayapi-302890064Nessuna valutazione finora
- Journal Reading - Myringitis - Elisabeth PattyDocumento14 pagineJournal Reading - Myringitis - Elisabeth PattyLipatOla123Nessuna valutazione finora
- PreparateDocumento2 paginePreparateVasile LozinschiiNessuna valutazione finora
- MDOC Sued For Handling of CoronavirusDocumento56 pagineMDOC Sued For Handling of CoronavirusTaylor DesOrmeau100% (1)
- Fulmer SPICES: An Overall Assessment Tool For Older AdultsDocumento2 pagineFulmer SPICES: An Overall Assessment Tool For Older AdultsSteve GarrettNessuna valutazione finora
- 15 English PPT Nursing 5 ADocumento208 pagine15 English PPT Nursing 5 ASinta WuLandari100% (1)
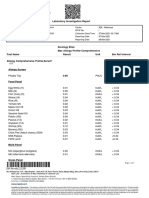
- Laboratory Investigation ReportDocumento7 pagineLaboratory Investigation ReportAmarjeetNessuna valutazione finora
- Pain Fellowship ProgramDocumento14 paginePain Fellowship ProgramshahidkhattakNessuna valutazione finora
- STI AwarenessDocumento7 pagineSTI AwarenessMarcus RossNessuna valutazione finora
- Practice Worksheet Class XiiDocumento7 paginePractice Worksheet Class XiiManjusha NayakNessuna valutazione finora
- Prenatal and Postpartum Aromatherapy ResourcesDocumento2 paginePrenatal and Postpartum Aromatherapy Resourcescansu sezerNessuna valutazione finora
- Jurnal PterigiumDocumento6 pagineJurnal PterigiumMonica Lauretta Sembiring IINessuna valutazione finora
- Participant Final Exam Answer Sheet: Emergency First Response Primary Care (CPR)Documento2 pagineParticipant Final Exam Answer Sheet: Emergency First Response Primary Care (CPR)Zirak Maan HussamiNessuna valutazione finora
- Case Report: Hepatitis BDocumento34 pagineCase Report: Hepatitis Bdewi sartikaNessuna valutazione finora
- Sarcomas of The Head and Neck: Dr. DarwitoDocumento60 pagineSarcomas of The Head and Neck: Dr. DarwitolaurasheerNessuna valutazione finora
- Basic Medical Sign LanguageDocumento8 pagineBasic Medical Sign LanguageRohan Kurade100% (1)
- CONJUNCTIVITIS or Pink Eye, Emotional and Spiritual MeaningDocumento1 paginaCONJUNCTIVITIS or Pink Eye, Emotional and Spiritual MeaningSarah g.Nessuna valutazione finora
- NUR194 ADocumento15 pagineNUR194 AJemuel DalanaNessuna valutazione finora
- Tetanus and Tetanus ToxoidDocumento24 pagineTetanus and Tetanus ToxoidFikar MajidNessuna valutazione finora
- FDG PET - CT-based Response AssessmentDocumento17 pagineFDG PET - CT-based Response AssessmentHelen MejiaNessuna valutazione finora
- Management of Acute Glomerulonephritis in Children: Children's Services Medical GuidelinesDocumento7 pagineManagement of Acute Glomerulonephritis in Children: Children's Services Medical GuidelinesdaypranitaNessuna valutazione finora
- FP Form ItrDocumento2 pagineFP Form ItrAlibasher Macalnas100% (1)
- Prosthetic Case PresentationsDocumento19 pagineProsthetic Case PresentationsptannenbaumNessuna valutazione finora
- Indications and Short-Term Outcome of Major Lower Extremity Amputations in Khartoum Teaching HospitalDocumento8 pagineIndications and Short-Term Outcome of Major Lower Extremity Amputations in Khartoum Teaching Hospitaljean vargasNessuna valutazione finora