Potrebbero piacerti anche
- S 055 LBLDocumento14 pagineS 055 LBLFranz Josef TariganNessuna valutazione finora
- Opioid Dose Equivalence: Calculation of Oral Morphine Equivalent Daily Dose (oMEDD)Documento3 pagineOpioid Dose Equivalence: Calculation of Oral Morphine Equivalent Daily Dose (oMEDD)Franz Josef TariganNessuna valutazione finora
- New Zealand Data Sheet: OXYNORM® Capsules OXYNORM® Oral SolutionDocumento14 pagineNew Zealand Data Sheet: OXYNORM® Capsules OXYNORM® Oral SolutionFranz Josef TariganNessuna valutazione finora
- Nutrition and DietDocumento26 pagineNutrition and DietadsfsdfNessuna valutazione finora
- S 015 LBLDocumento30 pagineS 015 LBLFranz Josef TariganNessuna valutazione finora
- Pengaruh Puasa Selama Ramadan Terhadap Status Klinik Penderita Diabetes Melitus Tipe 2Documento5 paginePengaruh Puasa Selama Ramadan Terhadap Status Klinik Penderita Diabetes Melitus Tipe 2Maulana MalikNessuna valutazione finora
- Oxynorm 5Mg Capsules / Oxycodone Hydrochloride 5Mg CapsulesDocumento2 pagineOxynorm 5Mg Capsules / Oxycodone Hydrochloride 5Mg CapsulesFranz Josef TariganNessuna valutazione finora
- Mechanical VentDocumento24 pagineMechanical VentRochim CoolNessuna valutazione finora
- S 020 LBLDocumento2 pagineS 020 LBLFranz Josef TariganNessuna valutazione finora
- Comparative Time Achieved VAS 3 On Oxycodone and Fentanyl Intravenous Continue As Post-Operative AnalgesiaDocumento3 pagineComparative Time Achieved VAS 3 On Oxycodone and Fentanyl Intravenous Continue As Post-Operative AnalgesiaFranz Josef TariganNessuna valutazione finora
- Tarigan Franz JDocumento3 pagineTarigan Franz JFranz Josef TariganNessuna valutazione finora
- Antibiotic ChoicesDocumento57 pagineAntibiotic ChoicestmleNessuna valutazione finora
- Bupivacaine Merk 4Documento2 pagineBupivacaine Merk 4PutuNessuna valutazione finora
- New Zealand Data Sheet: OXYNORM® Capsules OXYNORM® Oral SolutionDocumento14 pagineNew Zealand Data Sheet: OXYNORM® Capsules OXYNORM® Oral SolutionFranz Josef TariganNessuna valutazione finora
- BackgroundDocumento2 pagineBackgroundFranz Josef TariganNessuna valutazione finora
- New Zealand Data Sheet: OXYNORM® Capsules OXYNORM® Oral SolutionDocumento14 pagineNew Zealand Data Sheet: OXYNORM® Capsules OXYNORM® Oral SolutionFranz Josef TariganNessuna valutazione finora
- S 059 LBLDocumento30 pagineS 059 LBLFranz Josef TariganNessuna valutazione finora
- Characteristic of Calories Intake Dan Blood Glucose Profile On Ramadhan Fasting and Non Fasting People With Diabetes Mellitus IIDocumento9 pagineCharacteristic of Calories Intake Dan Blood Glucose Profile On Ramadhan Fasting and Non Fasting People With Diabetes Mellitus IIFranz Josef TariganNessuna valutazione finora
- Pengaruh Puasa Selama Ramadan Terhadap Status Klinik Penderita Diabetes Melitus Tipe 2Documento5 paginePengaruh Puasa Selama Ramadan Terhadap Status Klinik Penderita Diabetes Melitus Tipe 2Maulana MalikNessuna valutazione finora
- MorphineDocumento4 pagineMorphineMARITIM GEOFFREY KIPLANGATNessuna valutazione finora
- CRRT Antibiotic DosingDocumento8 pagineCRRT Antibiotic DosingFranz Josef TariganNessuna valutazione finora
- CRRT and AntibioticsDocumento8 pagineCRRT and Antibiotics491970Nessuna valutazione finora
- Paper No 60 EACEF 2017 PDFDocumento8 paginePaper No 60 EACEF 2017 PDFFranz Josef TariganNessuna valutazione finora
- S 059 LBLDocumento30 pagineS 059 LBLFranz Josef TariganNessuna valutazione finora
- 842 Erskine MythsDocumento3 pagine842 Erskine MythsFranz Josef TariganNessuna valutazione finora
- BackgroundDocumento2 pagineBackgroundFranz Josef TariganNessuna valutazione finora
- Anestesi Pada Pasien Dengan Penyakit Sistem KVDocumento13 pagineAnestesi Pada Pasien Dengan Penyakit Sistem KVFranz Josef TariganNessuna valutazione finora
- 2 Feb ICU Stroke Hemoragik AWDocumento15 pagine2 Feb ICU Stroke Hemoragik AWFranz Josef TariganNessuna valutazione finora
- Boarding Pass BerangkatDocumento6 pagineBoarding Pass BerangkatFranz Josef TariganNessuna valutazione finora
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (344)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (399)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (588)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (73)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2259)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (120)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- Pocket MedicineDocumento10 paginePocket MedicinePrasoot Suksombut14% (22)
- DR Vincet Raj Poul, Conulstant-AnesthesiaDocumento3 pagineDR Vincet Raj Poul, Conulstant-AnesthesiaKUMARJIT SAHANessuna valutazione finora
- Frozen ShoulderDocumento4 pagineFrozen Shoulderjimitkapadia100% (1)
- Unit 0000 Word Association 1: Missing Links: For Reference See A & C Black Dictionary of Medical Terms (0 7136 7603 5)Documento16 pagineUnit 0000 Word Association 1: Missing Links: For Reference See A & C Black Dictionary of Medical Terms (0 7136 7603 5)ahmad baihaqiNessuna valutazione finora
- Job Satisfaction On Nursing Student of UPHSD-Cal Batches 2006-2008Documento13 pagineJob Satisfaction On Nursing Student of UPHSD-Cal Batches 2006-2008Joshua PascasioNessuna valutazione finora
- RS. Premier Bintaro Pathology Service RS. Premier Bintaro Pathology ServiceDocumento1 paginaRS. Premier Bintaro Pathology Service RS. Premier Bintaro Pathology Serviceintan riniNessuna valutazione finora
- 365 ESL Short StoriesDocumento122 pagine365 ESL Short StoriesCarla Airam GreyNessuna valutazione finora
- Unit Test 2BDocumento2 pagineUnit Test 2BSantiago Contreras0% (1)
- Scope of Nle825Documento131 pagineScope of Nle825ericNessuna valutazione finora
- 3 RelationalmodelDocumento49 pagine3 RelationalmodelPengkuh Ardi NugrahaNessuna valutazione finora
- Dynamic Psychotherapy PDFDocumento603 pagineDynamic Psychotherapy PDFfllorinv775% (4)
- The GWAC Critical Care Chronicle 6-14Documento5 pagineThe GWAC Critical Care Chronicle 6-14gwacaacnNessuna valutazione finora
- Principles of Safe SurgeryDocumento19 paginePrinciples of Safe SurgeryGideon K. MutaiNessuna valutazione finora
- Design 1 Plans-ModelDocumento1 paginaDesign 1 Plans-ModelKinjal HarpavatNessuna valutazione finora
- The Impact of Human Resources Management On Healthcare QualityDocumento10 pagineThe Impact of Human Resources Management On Healthcare Qualityveerji007Nessuna valutazione finora
- Rec To Vaginal Fistula RepairDocumento7 pagineRec To Vaginal Fistula Repairnaftalina7Nessuna valutazione finora
- Adult Physiatric History and ExaminationDocumento11 pagineAdult Physiatric History and Examinationsylschebe22gmailNessuna valutazione finora
- FY2 Post QuestionsDocumento5 pagineFY2 Post QuestionsRohini Selvarajah67% (3)
- An Ideal ICU: Yogasliana FathudinDocumento16 pagineAn Ideal ICU: Yogasliana FathudinyogasNessuna valutazione finora
- Harmony Magazine, Volume 8 (2006-2007)Documento96 pagineHarmony Magazine, Volume 8 (2006-2007)UofACOMNessuna valutazione finora
- Research Outline - Universal HealthcareDocumento8 pagineResearch Outline - Universal HealthcarenemellistxNessuna valutazione finora
- Drug Study: Phinma University of PangasinanDocumento1 paginaDrug Study: Phinma University of PangasinanVoid LessNessuna valutazione finora
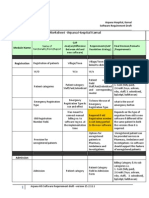
- Finalized Requirements-Worksheet - Arpana Hospital KarnalDocumento11 pagineFinalized Requirements-Worksheet - Arpana Hospital KarnalMahesh PatilNessuna valutazione finora
- Barrett Impulsiveness Scale (BIS-11)Documento10 pagineBarrett Impulsiveness Scale (BIS-11)andr3yl0Nessuna valutazione finora
- ASPE Vol3 Chapter2 PDFDocumento56 pagineASPE Vol3 Chapter2 PDFAu C. GacotNessuna valutazione finora
- 2005step3 IntroductionDocumento91 pagine2005step3 Introductioncalven82100% (1)
- Christmas in PragueDocumento2 pagineChristmas in PragueWestEnglishInstituteNessuna valutazione finora
- Hamida Haron CaseDocumento5 pagineHamida Haron CasegadzNessuna valutazione finora
- Hospital Application Guide SchneiderDocumento51 pagineHospital Application Guide SchneiderSundaresan SabanayagamNessuna valutazione finora
- Hua Nan Commercial Bank: More PlacesDocumento2 pagineHua Nan Commercial Bank: More Placesgodofredo dumaliNessuna valutazione finora