Potrebbero piacerti anche
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (895)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (121)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (74)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
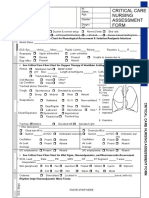
- Idoc - Pub - Critical Care Nursing Assessment FormDocumento3 pagineIdoc - Pub - Critical Care Nursing Assessment FormNamra AnsariNessuna valutazione finora
- Lung Dissection Lab ReportDocumento10 pagineLung Dissection Lab ReportSantiago MacíasNessuna valutazione finora
- J1 - 0104 0707 Tce 25 01 0220015Documento8 pagineJ1 - 0104 0707 Tce 25 01 0220015أحمد نور الهدايةNessuna valutazione finora
- Sci Med J 1990 2 4 87Documento14 pagineSci Med J 1990 2 4 87أحمد نور الهدايةNessuna valutazione finora
- Connection Between Allergic Rhinitis, Asma and SinusitisDocumento4 pagineConnection Between Allergic Rhinitis, Asma and Sinusitisأحمد نور الهدايةNessuna valutazione finora
- Septum MigrenDocumento6 pagineSeptum Migrenأحمد نور الهدايةNessuna valutazione finora
- Jazzle George E. Oteyza NCMB 312 Rle BSN 3Y1-3A Lab Module Course TaskDocumento3 pagineJazzle George E. Oteyza NCMB 312 Rle BSN 3Y1-3A Lab Module Course TaskwokorowNessuna valutazione finora
- Coronary Artery DiseaseDocumento110 pagineCoronary Artery DiseaseMaesy Garcia LorenaNessuna valutazione finora
- Surgical Correction Subglottic Stenosis of The Larynx: AnnoldDocumento6 pagineSurgical Correction Subglottic Stenosis of The Larynx: Annoldcanndy202Nessuna valutazione finora
- Anatomy Notes 2Documento105 pagineAnatomy Notes 2John SmithNessuna valutazione finora
- Drugs, Discussion On IGCSE Past PaperDocumento9 pagineDrugs, Discussion On IGCSE Past PaperinadirahNessuna valutazione finora
- Atlas of Flexible BronchosDocumento252 pagineAtlas of Flexible BronchosDenniszá Kósa100% (2)
- Performing Nasopharyngeal/Nasotracheal Suctioning Purposes:: Excellent Very Good Good Fair PoorDocumento6 paginePerforming Nasopharyngeal/Nasotracheal Suctioning Purposes:: Excellent Very Good Good Fair PoorJmarie Brillantes PopiocoNessuna valutazione finora
- Corpus Alienum EsophagusDocumento3 pagineCorpus Alienum EsophagusTrhey Ahmilza DamaitaNessuna valutazione finora
- Breathing and ExchangeDocumento40 pagineBreathing and ExchangeShambhaviNessuna valutazione finora
- 1a - Gonzalez, Jamaica Caryl N. (Respiratory)Documento13 pagine1a - Gonzalez, Jamaica Caryl N. (Respiratory)Jhamm GonzalezNessuna valutazione finora
- 2021 - 2022 Tracheostomy Care ProcedureDocumento69 pagine2021 - 2022 Tracheostomy Care ProcedureMelinda Cariño BallonNessuna valutazione finora
- Test Bank For Database Concepts 6th Edition KroenkeDocumento24 pagineTest Bank For Database Concepts 6th Edition KroenkeJasonFitzpatrickozyb100% (39)
- Aula 1 - Tracheobronchial BranchingDocumento16 pagineAula 1 - Tracheobronchial BranchingThiago StoianovNessuna valutazione finora
- Human Body Heroes-Discover San Miguel Leyte!Documento29 pagineHuman Body Heroes-Discover San Miguel Leyte!Hardy MisagalNessuna valutazione finora
- Undergraduate Ent Radiology: Dr. Davis Thomas PulimoottilDocumento41 pagineUndergraduate Ent Radiology: Dr. Davis Thomas PulimoottilAsif AbbasNessuna valutazione finora
- Small Animal Medicine Upper Airways ChartsDocumento14 pagineSmall Animal Medicine Upper Airways ChartsBrookeNessuna valutazione finora
- General Science Paper - I & II (English - Medium)Documento8 pagineGeneral Science Paper - I & II (English - Medium)Linus Babu DasariNessuna valutazione finora
- Fundamentos de Auscultacion Pulmonar NEJM PDFDocumento8 pagineFundamentos de Auscultacion Pulmonar NEJM PDFMaría Fernanda RíosNessuna valutazione finora
- Anesthesia of The PigDocumento19 pagineAnesthesia of The PigJuan Fernando Calcina IsiqueNessuna valutazione finora
- Palliative Care - Overview of Cough, Stridor, and Hemoptysis - UpToDateDocumento19 paginePalliative Care - Overview of Cough, Stridor, and Hemoptysis - UpToDateThaísa NogueiraNessuna valutazione finora
- Functions of The Respiratory SystemDocumento10 pagineFunctions of The Respiratory Systemadelina.jianu9991Nessuna valutazione finora
- Consenso EUR TQTDocumento12 pagineConsenso EUR TQTCamila Villalobos BravoNessuna valutazione finora
- AirwayDocumento1 paginaAirwaykushishaNessuna valutazione finora
- Module 4 Respiratory SystemDocumento8 pagineModule 4 Respiratory SystemJake Donely C. PaduaNessuna valutazione finora
- Science 9 Module 1 Week 1 PDFDocumento26 pagineScience 9 Module 1 Week 1 PDFMarco Angelo Lebios86% (7)
- JR Farlar 6Documento5 pagineJR Farlar 6Coryza Gabrie tanNessuna valutazione finora
- Role of X-Rays in OtolaryngolgoyDocumento25 pagineRole of X-Rays in OtolaryngolgoyDr. T. Balasubramanian67% (3)
- Respiratory Notes (Chris Andersen, ICUPrimaryPrep - Com)Documento14 pagineRespiratory Notes (Chris Andersen, ICUPrimaryPrep - Com)PkernNessuna valutazione finora