Potrebbero piacerti anche
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- BOCS PPSA Deed of Charge Over Deposit (Clean) (2012)Documento36 pagineBOCS PPSA Deed of Charge Over Deposit (Clean) (2012)Energyte BaldonadoNessuna valutazione finora
- SFA15G01S339Extraterritoriality Amendments 2014Documento14 pagineSFA15G01S339Extraterritoriality Amendments 2014Energyte BaldonadoNessuna valutazione finora
- How To Raise Money On A Blockchain With A TokenDocumento12 pagineHow To Raise Money On A Blockchain With A TokenEnergyte BaldonadoNessuna valutazione finora
- 2018PressRelease Draft ICO Rules August 02 2018 1Documento3 pagine2018PressRelease Draft ICO Rules August 02 2018 1Energyte BaldonadoNessuna valutazione finora
- Sec Memo 01, s2009Documento6 pagineSec Memo 01, s2009Energyte BaldonadoNessuna valutazione finora
- RA 5921 Regulates Pharmacy Practice & Education StandardsDocumento14 pagineRA 5921 Regulates Pharmacy Practice & Education StandardsSunshine_Bacla_4275100% (1)
- RA 8172 - Asin Law - 2Documento22 pagineRA 8172 - Asin Law - 2Maxine Alexandra JaimeNessuna valutazione finora
- RA 2382 The Medical Act of 1959Documento18 pagineRA 2382 The Medical Act of 1959Simon James SemillaNessuna valutazione finora
- RA 4419 The Philippine Dental Act of 1965Documento13 pagineRA 4419 The Philippine Dental Act of 1965Energyte BaldonadoNessuna valutazione finora
- RA 9178 BMBE ActDocumento69 pagineRA 9178 BMBE Actinvictusinc100% (1)
- RA 8976 - Food Fortification Law - RevisedDocumento4 pagineRA 8976 - Food Fortification Law - RevisedTim Alvaran100% (1)
- RA 10620 (Toy and Game Safety Labeling Act of 2013)Documento4 pagineRA 10620 (Toy and Game Safety Labeling Act of 2013)Energyte BaldonadoNessuna valutazione finora
- RA 10747 - Rare Disease ActDocumento7 pagineRA 10747 - Rare Disease ActEnergyte BaldonadoNessuna valutazione finora
- The Use of Genomic InformationDocumento3 pagineThe Use of Genomic InformationEnergyte BaldonadoNessuna valutazione finora
- Investment MemorandumDocumento17 pagineInvestment MemorandumEnergyte BaldonadoNessuna valutazione finora
- Drive Discovery With Most Complete View of Cancer ComplexityDocumento2 pagineDrive Discovery With Most Complete View of Cancer ComplexityEnergyte BaldonadoNessuna valutazione finora
- New Course Layout Skate TownDocumento10 pagineNew Course Layout Skate TownEnergyte BaldonadoNessuna valutazione finora
- PWC Doing Business in The Netherlands 2017 PDFDocumento52 paginePWC Doing Business in The Netherlands 2017 PDFEnergyte BaldonadoNessuna valutazione finora
- Genomic Research and Human Subject PrivacyDocumento11 pagineGenomic Research and Human Subject PrivacyEnergyte BaldonadoNessuna valutazione finora
- Reit Law Republic Act 9856Documento25 pagineReit Law Republic Act 9856Leonardo MagnawaNessuna valutazione finora
- Impeachment Complaint Example 2008 November PGMADocumento103 pagineImpeachment Complaint Example 2008 November PGMAEnergyte BaldonadoNessuna valutazione finora
- Sample Drug Free Workplace Policy Program 02 July 2013Documento9 pagineSample Drug Free Workplace Policy Program 02 July 2013Energyte BaldonadoNessuna valutazione finora
- DNA Sequencing MethodsDocumento23 pagineDNA Sequencing MethodsNT VivekNessuna valutazione finora
- Mutual Fund Statistics Oct2004 PhilippinesDocumento1 paginaMutual Fund Statistics Oct2004 PhilippinesEnergyte BaldonadoNessuna valutazione finora
- Estate Settlement GuidelinesDocumento4 pagineEstate Settlement GuidelinesOfel TactacNessuna valutazione finora
- Sample Drug Free Workplace Policy ProgramDocumento9 pagineSample Drug Free Workplace Policy ProgramEnergyte BaldonadoNessuna valutazione finora
- Private Placement Bonds-A Valuable AlternativeDocumento6 paginePrivate Placement Bonds-A Valuable AlternativeEnergyte BaldonadoNessuna valutazione finora
- 10 Things The Best Law Firm Website Designs Have in CommonDocumento14 pagine10 Things The Best Law Firm Website Designs Have in CommonEnergyte BaldonadoNessuna valutazione finora
- Template For The Articles of Incorporation of A Non-Stock Non-Profit Philippine CorporationDocumento9 pagineTemplate For The Articles of Incorporation of A Non-Stock Non-Profit Philippine CorporationEnergyte Baldonado0% (2)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (890)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (587)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (399)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (344)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (73)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (265)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2219)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (119)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
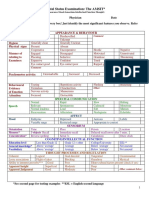
- Mental Status Examination: The AMSIT : Neat and Tidy DisshevelledDocumento2 pagineMental Status Examination: The AMSIT : Neat and Tidy Disshevellednisreen100% (1)
- LeprosyDocumento9 pagineLeprosyJohn Ribu Parampil100% (1)
- Guidelines For The Use of RH (D) Immunoglobulin (Anti D) (C Obs 6) Review November 2015Documento11 pagineGuidelines For The Use of RH (D) Immunoglobulin (Anti D) (C Obs 6) Review November 2015vasanthNessuna valutazione finora
- Preceptorship Journal 2Documento3 paginePreceptorship Journal 2api-325099570Nessuna valutazione finora
- MCMI-IV Interpretive Report - 6856501 - 20180509033028436 PDFDocumento10 pagineMCMI-IV Interpretive Report - 6856501 - 20180509033028436 PDFChristianJ.Rodriguez100% (1)
- GLUCOSE TOLERANCE TEST GUIDEDocumento12 pagineGLUCOSE TOLERANCE TEST GUIDEshiv gautamNessuna valutazione finora
- Medical Devices by FacilityDocumento60 pagineMedical Devices by FacilityjwalitNessuna valutazione finora
- Prevention of Odontogenic Infection - Principles of Management - Dental Ebook & Lecture Notes PDF Download (Studynama - Com - India's Biggest Website For BDS Study Material Downloads)Documento17 paginePrevention of Odontogenic Infection - Principles of Management - Dental Ebook & Lecture Notes PDF Download (Studynama - Com - India's Biggest Website For BDS Study Material Downloads)Vinnie SinghNessuna valutazione finora
- Chapter 18 Personality DisordersDocumento10 pagineChapter 18 Personality DisordersCatia Fernandes100% (2)
- Lecture 4 Medical Terminology PDFDocumento38 pagineLecture 4 Medical Terminology PDFAhmed KhaledNessuna valutazione finora
- Kodak Dental 1 Successful Panoramic RadiographyDocumento24 pagineKodak Dental 1 Successful Panoramic Radiographymanishbabu100% (2)
- Cleft Lip or Cleft Palate / Pharyngoplasty Clinical Pathway: Personal DetailsDocumento8 pagineCleft Lip or Cleft Palate / Pharyngoplasty Clinical Pathway: Personal DetailsRegine LacosteNessuna valutazione finora
- Cluster A Personality DisordersDocumento2 pagineCluster A Personality Disordersxerah0808Nessuna valutazione finora
- Antimicrobial ChemotherapyDocumento160 pagineAntimicrobial Chemotherapyokumu atanas0% (1)
- Principles of Behavior ChangeDocumento10 paginePrinciples of Behavior ChangeGuillermo ThomasNessuna valutazione finora
- Coley 2019Documento8 pagineColey 2019KaniNessuna valutazione finora
- Oxy CadDocumento21 pagineOxy CadrlinaoNessuna valutazione finora
- Constrictive Pericarditis - UpToDateDocumento26 pagineConstrictive Pericarditis - UpToDateSebastian CastañedaNessuna valutazione finora
- Venous Thromboembolism in Pregnancy: Risks, Diagnosis and TreatmentDocumento10 pagineVenous Thromboembolism in Pregnancy: Risks, Diagnosis and Treatmentdr.diverNessuna valutazione finora
- Acoustic NeuromaDocumento6 pagineAcoustic NeuromayoghaNessuna valutazione finora
- Acute Service Pain Handbook 2011Documento116 pagineAcute Service Pain Handbook 2011Iskandar414Nessuna valutazione finora
- CLOZE TEST Discovery Could Ease Blood ShortageDocumento2 pagineCLOZE TEST Discovery Could Ease Blood ShortageKarsan Ayaz MaierNessuna valutazione finora
- Newborn Care PresentationDocumento35 pagineNewborn Care PresentationChristian PallaviNessuna valutazione finora
- Ross Case Book 2016Documento305 pagineRoss Case Book 2016S86% (7)
- Micro Cystic AcneDocumento2 pagineMicro Cystic AcneNurul SalmaNessuna valutazione finora
- Calista Roy LuigiDocumento22 pagineCalista Roy LuigiLuigi Prada GuzmanNessuna valutazione finora
- Bionator: The Father of Functional OrthodonticsDocumento307 pagineBionator: The Father of Functional OrthodonticsApurava Singh100% (3)
- Janie Jacobs Resume March 2019Documento2 pagineJanie Jacobs Resume March 2019api-404179099Nessuna valutazione finora
- Nurs FPX 4020 Assessment 2 Root Cause Analysis and Safety Improvement PlanDocumento5 pagineNurs FPX 4020 Assessment 2 Root Cause Analysis and Safety Improvement PlanEmma WatsonNessuna valutazione finora