Potrebbero piacerti anche
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5782)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (399)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (587)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (72)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (344)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (119)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- Group A (Week 6) - Bisdig PDFDocumento14 pagineGroup A (Week 6) - Bisdig PDFAvilia Nurul SafitriNessuna valutazione finora
- CTT DE LOS ANDES LANGUAGE CENTER WORK GROUP – Waste Disposal reportDocumento7 pagineCTT DE LOS ANDES LANGUAGE CENTER WORK GROUP – Waste Disposal reportRosa CapeloNessuna valutazione finora
- Tle-Computer Systems SERVICING (Grade 10) : First Quarter - Module 1 Elements of ComputerDocumento9 pagineTle-Computer Systems SERVICING (Grade 10) : First Quarter - Module 1 Elements of ComputerQuerl Manzano SarabiaNessuna valutazione finora
- 00 EAN Abstract 2016 BookDocumento956 pagine00 EAN Abstract 2016 BookAlexandra MardareNessuna valutazione finora
- Project Requisition Format - Graduation Project - PEOPLE 3Documento2 pagineProject Requisition Format - Graduation Project - PEOPLE 3Jashid HameedNessuna valutazione finora
- Competency Log EC-12 Interactive ChartDocumento24 pagineCompetency Log EC-12 Interactive ChartNathan MeeceNessuna valutazione finora
- 12th Five - Year Plan 2012 - 2017Documento3 pagine12th Five - Year Plan 2012 - 2017workingaboNessuna valutazione finora
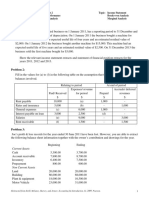
- Income Statement TutorialDocumento5 pagineIncome Statement TutorialKhiren MenonNessuna valutazione finora
- RED BULL - Marketing Success Report FINALDocumento12 pagineRED BULL - Marketing Success Report FINALvwuthooNessuna valutazione finora
- Irjet V6i4986Documento5 pagineIrjet V6i4986Uvesh ShaikhNessuna valutazione finora
- Vol II Tech Spec Sct1367Documento490 pagineVol II Tech Spec Sct1367ashish.mathur1Nessuna valutazione finora
- Scope of Work - Flow Line SurveyDocumento2 pagineScope of Work - Flow Line SurveyrutujaNessuna valutazione finora
- Systems Analysis and Design Feasibility Study TypesDocumento34 pagineSystems Analysis and Design Feasibility Study TypesMr.Nigght FuryNessuna valutazione finora
- Eve Ross - 10.3a - Note - Images in Concave MirrorsDocumento8 pagineEve Ross - 10.3a - Note - Images in Concave MirrorsEve RossNessuna valutazione finora
- CV For UnescoDocumento6 pagineCV For UnescoArpan BhujuNessuna valutazione finora
- Basell PP Homo Rafia Hp456j Mi 3 4Documento2 pagineBasell PP Homo Rafia Hp456j Mi 3 4crawn06Nessuna valutazione finora
- Passengers' Perspective of Philippine Airlines Within Nueva EcijaDocumento15 paginePassengers' Perspective of Philippine Airlines Within Nueva EcijaPoonam KilaniyaNessuna valutazione finora
- MECHANICAL PROCESS ENGINEERING STORAGE AND FLOW OF BULK SOLIDSDocumento1 paginaMECHANICAL PROCESS ENGINEERING STORAGE AND FLOW OF BULK SOLIDSEstefanía Gómez RodríguezNessuna valutazione finora
- Timss & Pisa Models: Khalidah AhmadDocumento51 pagineTimss & Pisa Models: Khalidah AhmadMirahmad FadzlyNessuna valutazione finora
- Formulation and Testing of Herbal Syrup For Cough and AsthmaDocumento11 pagineFormulation and Testing of Herbal Syrup For Cough and Asthmanaomiesolefack03Nessuna valutazione finora
- City Union Bank Inspection ReportDocumento114 pagineCity Union Bank Inspection ReportMoneylife Foundation100% (1)
- Golar Viking Case Study NSFMWDocumento7 pagineGolar Viking Case Study NSFMWMatteo ConciNessuna valutazione finora
- Development Information: KEB Info Specifications of The HSP5-InterfaceDocumento3 pagineDevelopment Information: KEB Info Specifications of The HSP5-Interfacewaqasasad408Nessuna valutazione finora
- Module 3 - Topic 3Documento4 pagineModule 3 - Topic 3Moon LightNessuna valutazione finora
- Alveolar Bone DR DeepakDocumento107 pagineAlveolar Bone DR DeepakDeepak Kumar100% (2)
- Test Questions GRADE 9 NAIL CAREDocumento2 pagineTest Questions GRADE 9 NAIL CARESharmaine ManigosNessuna valutazione finora
- Soil Components: The Role of Air and Water in Soil Pore SpacesDocumento9 pagineSoil Components: The Role of Air and Water in Soil Pore SpacesJohn Lester AlforteNessuna valutazione finora
- Carto 3 System OverviewDocumento8 pagineCarto 3 System Overviewdanang setiawanNessuna valutazione finora
- Anemia ProjectDocumento33 pagineAnemia ProjectNilesh BagalNessuna valutazione finora
- Furuno SC-50 - 110Documento30 pagineFuruno SC-50 - 110etchegarayf100% (1)