Potrebbero piacerti anche
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5784)
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (890)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (399)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (72)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (344)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (119)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- 11-Testicular-Cancer 2017 WebDocumento56 pagine11-Testicular-Cancer 2017 WebagungratihNessuna valutazione finora
- A Precise Report On CancerDocumento34 pagineA Precise Report On CancerArnab ChakraborttyNessuna valutazione finora
- Medscape and RadiopediaDocumento21 pagineMedscape and RadiopediaRuhasri HumastutiNessuna valutazione finora
- LobectomyDocumento3 pagineLobectomyJrosejorge TaparNessuna valutazione finora
- Trường Đại Học Y Khoa Phạm Ngọc Thạch: Name: ClassDocumento45 pagineTrường Đại Học Y Khoa Phạm Ngọc Thạch: Name: ClassĐoàn Tuấn KhôiNessuna valutazione finora
- Vitamin D in Combination Cancer TreatmentDocumento17 pagineVitamin D in Combination Cancer TreatmentnendenNessuna valutazione finora
- Lung Cancer Principles and PracticeDocumento1 paginaLung Cancer Principles and PracticeOrlin ZlatarskiNessuna valutazione finora
- CANCER: A GUIDE TO THE DISEASE AND ITS TREATMENTSDocumento135 pagineCANCER: A GUIDE TO THE DISEASE AND ITS TREATMENTSEnzo TimbolNessuna valutazione finora
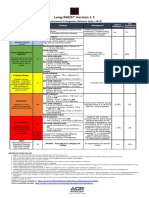
- Lung RADS® Version 1.1: Assessment Categories Release Date: 2019Documento1 paginaLung RADS® Version 1.1: Assessment Categories Release Date: 2019S Francisco MotNessuna valutazione finora
- CT Applications in Chest PathologyDocumento16 pagineCT Applications in Chest PathologyNilanka SandunNessuna valutazione finora
- Overview of evaluating, diagnosing, and staging suspected lung cancerDocumento197 pagineOverview of evaluating, diagnosing, and staging suspected lung cancerFernando HuertasNessuna valutazione finora
- Nejmcpc 1102202Documento10 pagineNejmcpc 1102202FrinkooFrinkoBNessuna valutazione finora
- Luminair PDFDocumento229 pagineLuminair PDFMohammed Shahin40% (5)
- Whole-Body FDG PET Imaging in OncologyDocumento305 pagineWhole-Body FDG PET Imaging in OncologyTurki100% (5)
- Presentation Small Cell Lung CancerDocumento59 paginePresentation Small Cell Lung Cancerprudhviraj mNessuna valutazione finora
- The Timely Delivery of Radical Radiotherapy: Guidelines For The Management of Unscheduled Treatment InterruptionsDocumento39 pagineThe Timely Delivery of Radical Radiotherapy: Guidelines For The Management of Unscheduled Treatment InterruptionsshreyaNessuna valutazione finora
- Cardinal Manifestations of CancerDocumento6 pagineCardinal Manifestations of CancerMaaz KhajaNessuna valutazione finora
- Lisbon 2015 Boa PDFDocumento477 pagineLisbon 2015 Boa PDFogespaikiNessuna valutazione finora
- Respiratory Medicine Case Reports: Henry W. Ainge-Allen, Paul A. Lilburn, Daniel Moses, Colin Chen, Paul S. ThomasDocumento3 pagineRespiratory Medicine Case Reports: Henry W. Ainge-Allen, Paul A. Lilburn, Daniel Moses, Colin Chen, Paul S. ThomasPauloCostaNessuna valutazione finora
- Zanki Respiratory PathologyDocumento15 pagineZanki Respiratory Pathologysmian08100% (1)
- Fresh potato juice shown to control cancer cell spreadDocumento12 pagineFresh potato juice shown to control cancer cell spreadlawnmawn100% (1)
- Severe Asthma-Pathogenesis and Clinical ManagementDocumento706 pagineSevere Asthma-Pathogenesis and Clinical ManagementNatia Demetradze0% (1)
- JKC Grand Test 1 - 2013Documento6 pagineJKC Grand Test 1 - 2013Surya NarayanaNessuna valutazione finora
- Quiz OncologyDocumento20 pagineQuiz OncologyJona Joyce JunsayNessuna valutazione finora
- Diagnostic Imaging and Procedures for Respiratory DiseaseDocumento41 pagineDiagnostic Imaging and Procedures for Respiratory DiseaseVio Mincu100% (1)
- NCI Validates Homoeopathic Cancer TreatmentDocumento6 pagineNCI Validates Homoeopathic Cancer TreatmentSuraj YadavNessuna valutazione finora
- Cancer NotesDocumento12 pagineCancer Noteswavezone113Nessuna valutazione finora
- Total Quit KitDocumento47 pagineTotal Quit Kitrahul.mishraNessuna valutazione finora
- John's Smoking ConfessionsDocumento5 pagineJohn's Smoking ConfessionsFrancisous Mee100% (1)
- Lesson Plan On Lung CancerDocumento10 pagineLesson Plan On Lung CancerPankaj Jena100% (1)