Potrebbero piacerti anche
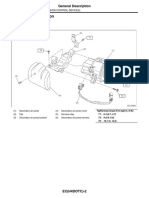
- Emission+Control+ (Aux +Emission+Control+Devices) + (H4DOTC)Documento27 pagineEmission+Control+ (Aux +Emission+Control+Devices) + (H4DOTC)Marcelo BedoyaNessuna valutazione finora
- Ubogu - Inflammatory NeuropathiesDocumento24 pagineUbogu - Inflammatory NeuropathiesMarcelo BedoyaNessuna valutazione finora
- Valadi - Guillain-Barré SyndromeDocumento5 pagineValadi - Guillain-Barré SyndromeMarcelo BedoyaNessuna valutazione finora
- Asbury - Assesment of Current Diagnostic Criteria For GBSDocumento4 pagineAsbury - Assesment of Current Diagnostic Criteria For GBSMarcelo BedoyaNessuna valutazione finora
- 2014 Fokke GBS Brighton Brain 2014Documento11 pagine2014 Fokke GBS Brighton Brain 2014Hikmat SatriaNessuna valutazione finora
- Pokemon: Opening Theme: XylophoneDocumento17 paginePokemon: Opening Theme: XylophoneMarcelo BedoyaNessuna valutazione finora
- 13 Patrick - Lead Toxicity - Exposure, Evaluation Adn TreatmentDocumento21 pagine13 Patrick - Lead Toxicity - Exposure, Evaluation Adn TreatmentMarcelo BedoyaNessuna valutazione finora
- +09 US Geological Survey - Mineral Commodity Summaries 2016Documento205 pagine+09 US Geological Survey - Mineral Commodity Summaries 2016Marcelo BedoyaNessuna valutazione finora
- CG54 MigratedDocumento34 pagineCG54 MigratedMarcelo BedoyaNessuna valutazione finora
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5795)
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (588)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (74)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (895)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (400)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (345)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2259)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (266)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (121)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- Eurocode 3: Design of Steel Structures "ReadyDocumento26 pagineEurocode 3: Design of Steel Structures "Readywazydotnet80% (10)
- Concrete Repair Manual (2017)Documento59 pagineConcrete Repair Manual (2017)Fernando EscriváNessuna valutazione finora
- TraceDocumento5 pagineTraceNorma TellezNessuna valutazione finora
- The Wayland News October 2014Documento16 pagineThe Wayland News October 2014Julian HornNessuna valutazione finora
- Lesson Plan For Implementing NETSDocumento5 pagineLesson Plan For Implementing NETSLisa PizzutoNessuna valutazione finora
- Lab Report SBK Sem 3 (Priscilla Tuyang)Documento6 pagineLab Report SBK Sem 3 (Priscilla Tuyang)Priscilla Tuyang100% (1)
- Ajmera - Treon - FF - R4 - 13-11-17 FinalDocumento45 pagineAjmera - Treon - FF - R4 - 13-11-17 FinalNikita KadamNessuna valutazione finora
- Arduino Uno CNC ShieldDocumento11 pagineArduino Uno CNC ShieldMărian IoanNessuna valutazione finora
- ALE Manual For LaserScope Arc Lamp Power SupplyDocumento34 pagineALE Manual For LaserScope Arc Lamp Power SupplyKen DizzeruNessuna valutazione finora
- Student Management SystemDocumento232 pagineStudent Management Systemslu_mangal73% (37)
- Pipe Cleaner Lesson PlanDocumento2 paginePipe Cleaner Lesson PlanTaylor FranklinNessuna valutazione finora
- Data StructuresDocumento4 pagineData StructuresBenjB1983Nessuna valutazione finora
- Hydraulic Mining ExcavatorDocumento8 pagineHydraulic Mining Excavatorasditia_07100% (1)
- Project Formulation and Appraisalpdf PDFDocumento12 pagineProject Formulation and Appraisalpdf PDFabhijeet varadeNessuna valutazione finora
- Computer Class 3 ThirdDocumento1 paginaComputer Class 3 ThirdbeakraamNessuna valutazione finora
- BLP#1 - Assessment of Community Initiative (3 Files Merged)Documento10 pagineBLP#1 - Assessment of Community Initiative (3 Files Merged)John Gladhimer CanlasNessuna valutazione finora
- ThorpeDocumento267 pagineThorpezaeem73Nessuna valutazione finora
- Statistics and Probability: Quarter 4 - (Week 6)Documento8 pagineStatistics and Probability: Quarter 4 - (Week 6)Jessa May MarcosNessuna valutazione finora
- Switching Simulation in GNS3 - GNS3Documento3 pagineSwitching Simulation in GNS3 - GNS3Jerry Fourier KemeNessuna valutazione finora
- CN1111 Tutorial 4 QuestionDocumento3 pagineCN1111 Tutorial 4 Questionthenewperson0% (1)
- Back Propagation Neural NetworkDocumento10 pagineBack Propagation Neural NetworkAhmad Bisyrul HafiNessuna valutazione finora
- Ilocos Norte Youth Development Office Accomplishment Report 2Documento17 pagineIlocos Norte Youth Development Office Accomplishment Report 2Solsona Natl HS MaanantengNessuna valutazione finora
- Mathematics BQP 2022Documento43 pagineMathematics BQP 2022muhammadmansuri815Nessuna valutazione finora
- RMC 102-2017 HighlightsDocumento3 pagineRMC 102-2017 HighlightsmmeeeowwNessuna valutazione finora
- Top Activist Stories - 5 - A Review of Financial Activism by Geneva PartnersDocumento8 pagineTop Activist Stories - 5 - A Review of Financial Activism by Geneva PartnersBassignotNessuna valutazione finora
- Binge Eating Disorder ANNADocumento12 pagineBinge Eating Disorder ANNAloloasbNessuna valutazione finora
- Mathematics Mock Exam 2015Documento4 pagineMathematics Mock Exam 2015Ian BautistaNessuna valutazione finora
- Эквивалентная Схема Мотра Теслы с Thomas2020Documento7 pagineЭквивалентная Схема Мотра Теслы с Thomas2020Алексей ЯмаNessuna valutazione finora
- Frellwits Swedish Hosts FileDocumento10 pagineFrellwits Swedish Hosts FileAnonymous DsGzm0hQf5Nessuna valutazione finora
- Blockchains: Architecture, Design and Use CasesDocumento26 pagineBlockchains: Architecture, Design and Use Caseseira kNessuna valutazione finora