Potrebbero piacerti anche
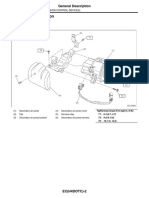
- Emission Control DevicesDocumento27 pagineEmission Control DevicesMarcelo BedoyaNessuna valutazione finora
- Music BooksDocumento1 paginaMusic BooksMarcelo BedoyaNessuna valutazione finora
- Lolli - Increased Reactivity To HTLV-1 in Inflammatory Nervous System DiseasesDocumento5 pagineLolli - Increased Reactivity To HTLV-1 in Inflammatory Nervous System DiseasesMarcelo BedoyaNessuna valutazione finora
- Karak - Pseudo GBS Masking Acute Myeloid Leukemia RelapseDocumento3 pagineKarak - Pseudo GBS Masking Acute Myeloid Leukemia RelapseMarcelo BedoyaNessuna valutazione finora
- Sejvar - GBS and Fisher Syndrome - Case Definitions and GuidelinesDocumento15 pagineSejvar - GBS and Fisher Syndrome - Case Definitions and GuidelinesMarcelo BedoyaNessuna valutazione finora
- Saito - Increased Expression of OX40 in HTLV-1 Associated MyelopathyDocumento15 pagineSaito - Increased Expression of OX40 in HTLV-1 Associated MyelopathyMarcelo BedoyaNessuna valutazione finora
- Valadi - Guillain-Barré SyndromeDocumento5 pagineValadi - Guillain-Barré SyndromeMarcelo BedoyaNessuna valutazione finora
- Kusumi - Epidemiology of Inflammatory Neurological and Inflamatory Neuromuscular Diseases in Tottori, JapanDocumento6 pagineKusumi - Epidemiology of Inflammatory Neurological and Inflamatory Neuromuscular Diseases in Tottori, JapanMarcelo BedoyaNessuna valutazione finora
- Uncini - 99 Years of Guillain Barre SyndromeDocumento2 pagineUncini - 99 Years of Guillain Barre SyndromeMarcelo BedoyaNessuna valutazione finora
- Ubogu - Inflammatory NeuropathiesDocumento24 pagineUbogu - Inflammatory NeuropathiesMarcelo BedoyaNessuna valutazione finora
- Abbi - Guillain-Barré Syndrome After Use of Alemtuzumab (Campath) in A Patient With HTLV-I With ATLL (Case Report)Documento3 pagineAbbi - Guillain-Barré Syndrome After Use of Alemtuzumab (Campath) in A Patient With HTLV-I With ATLL (Case Report)Marcelo BedoyaNessuna valutazione finora
- Brizzi - Peripheral Nerve in Infectious DiseasesDocumento12 pagineBrizzi - Peripheral Nerve in Infectious DiseasesMarcelo BedoyaNessuna valutazione finora
- Abbi - Guillain-Barré Syndrome After Use of Alemtuzumab (Campath) in A Patient With HTLV-I With ATLL (Case Report)Documento3 pagineAbbi - Guillain-Barré Syndrome After Use of Alemtuzumab (Campath) in A Patient With HTLV-I With ATLL (Case Report)Marcelo BedoyaNessuna valutazione finora
- Diagnostic Criteria for Guillain-Barré SyndromeDocumento4 pagineDiagnostic Criteria for Guillain-Barré SyndromeMarcelo BedoyaNessuna valutazione finora
- 20 Ronchetti - Lead Neurotoxicity in Children - Prenatal or Postnatal ExposureDocumento8 pagine20 Ronchetti - Lead Neurotoxicity in Children - Prenatal or Postnatal ExposureMarcelo BedoyaNessuna valutazione finora
- 2014 Fokke GBS Brighton Brain 2014Documento11 pagine2014 Fokke GBS Brighton Brain 2014Hikmat SatriaNessuna valutazione finora
- Guillian Barre SyndromeDocumento11 pagineGuillian Barre SyndromemohamedNessuna valutazione finora
- CDC Response Lead Exposure RecsDocumento16 pagineCDC Response Lead Exposure RecsAyu Wedhani SpcNessuna valutazione finora
- Pokemon: Opening Theme: XylophoneDocumento17 paginePokemon: Opening Theme: XylophoneMarcelo BedoyaNessuna valutazione finora
- Posibles Temas 2016 - IIDocumento1 paginaPosibles Temas 2016 - IIMarcelo BedoyaNessuna valutazione finora
- Pokémon Theme (2 Pianos)Documento7 paginePokémon Theme (2 Pianos)Marcelo BedoyaNessuna valutazione finora
- +09 US Geological Survey - Mineral Commodity Summaries 2016Documento205 pagine+09 US Geological Survey - Mineral Commodity Summaries 2016Marcelo BedoyaNessuna valutazione finora
- 18 - Schnaas - Reduced Intellectual Development in Children With Prenatal Lead ExposureDocumento7 pagine18 - Schnaas - Reduced Intellectual Development in Children With Prenatal Lead ExposureMarcelo BedoyaNessuna valutazione finora
- 13 Patrick - Lead Toxicity - Exposure, Evaluation Adn TreatmentDocumento21 pagine13 Patrick - Lead Toxicity - Exposure, Evaluation Adn TreatmentMarcelo BedoyaNessuna valutazione finora
- 02 WHO - Childhood Lead PoisoningDocumento74 pagine02 WHO - Childhood Lead PoisoningMarcelo BedoyaNessuna valutazione finora
- Guidelines 2012 2013Documento169 pagineGuidelines 2012 2013Marcelo BedoyaNessuna valutazione finora
- CG54 MigratedDocumento34 pagineCG54 MigratedMarcelo BedoyaNessuna valutazione finora
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5783)
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (890)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (399)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (72)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (344)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (119)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- Feasibility of Malunggay & Coconut Vinegar as Natural Cleaning AgentDocumento7 pagineFeasibility of Malunggay & Coconut Vinegar as Natural Cleaning AgentCharles Dave AvenidoNessuna valutazione finora
- BSHF-101 E.MDocumento8 pagineBSHF-101 E.MRajni KumariNessuna valutazione finora
- Surgery Final NotesDocumento81 pagineSurgery Final NotesDETECTIVE CONANNessuna valutazione finora
- 32 Vol4 EpaperDocumento32 pagine32 Vol4 EpaperThesouthasian TimesNessuna valutazione finora
- List of Pakistani Government Ministries and DivisionsDocumento2 pagineList of Pakistani Government Ministries and DivisionsbasitaleeNessuna valutazione finora
- Pencak Silat Talent ScoutDocumento9 paginePencak Silat Talent ScoutWisnu Bayu MurtiNessuna valutazione finora
- Jamaican Sprint SecretsDocumento37 pagineJamaican Sprint Secretspanthercoach54100% (2)
- Hubungan Pengetahuan Sikap Penderita Penyakit Malaria FalciparumDocumento63 pagineHubungan Pengetahuan Sikap Penderita Penyakit Malaria FalciparumEsty GulsanNessuna valutazione finora
- The Real Paul Thibault: Nothing But The Truth..Documento20 pagineThe Real Paul Thibault: Nothing But The Truth..LancasterFirstNessuna valutazione finora
- Kaplan Grade OverviewDocumento5 pagineKaplan Grade Overviewapi-310875630Nessuna valutazione finora
- Hazards of Dietary Supplement Use: Anthony E. Johnson, MD Chad A. Haley, MD John A. Ward, PHDDocumento10 pagineHazards of Dietary Supplement Use: Anthony E. Johnson, MD Chad A. Haley, MD John A. Ward, PHDJean CotteNessuna valutazione finora
- Pharmacology Mock Exam MCQDocumento8 paginePharmacology Mock Exam MCQanaeshklNessuna valutazione finora
- Portal Hypertension Clinical Features and ManagementDocumento29 paginePortal Hypertension Clinical Features and ManagementPhilip LingNessuna valutazione finora
- Research Paper For AbortionDocumento10 pagineResearch Paper For AbortionMarevisha Vidfather75% (4)
- PEMEDocumento1 paginaPEMERajesh MohananNessuna valutazione finora
- Sdera Demo Lesson DVD Worksheet 2021Documento2 pagineSdera Demo Lesson DVD Worksheet 2021api-396577001Nessuna valutazione finora
- Self Safety 2Documento10 pagineSelf Safety 2Angela MacailaoNessuna valutazione finora
- Handbook of Laboratory Animal Science - Vol IIIDocumento319 pagineHandbook of Laboratory Animal Science - Vol IIICarlos AlmeidaNessuna valutazione finora
- Tradition With A Future: Solutions For Operative HysterosDocumento16 pagineTradition With A Future: Solutions For Operative Hysterosأحمد قائدNessuna valutazione finora
- Biogas (Methane) EnglishDocumento8 pagineBiogas (Methane) Englishveluthambi8888100% (1)
- Syllabus ECDO 4225 - Professional Aspects of Nutrition and DieteticsDocumento6 pagineSyllabus ECDO 4225 - Professional Aspects of Nutrition and DieteticsOEAENessuna valutazione finora
- As 2550.5-2002 Cranes Hoists and Winches - Safe Use Mobile CranesDocumento8 pagineAs 2550.5-2002 Cranes Hoists and Winches - Safe Use Mobile CranesSAI Global - APACNessuna valutazione finora
- Hypertension Drugs Cheat Sheet: by ViaDocumento3 pagineHypertension Drugs Cheat Sheet: by ViaGulzaib KhokharNessuna valutazione finora
- Radiographic Cardiopulmonary Changes in Dogs With Heartworm DiseaseDocumento8 pagineRadiographic Cardiopulmonary Changes in Dogs With Heartworm DiseaseputriwilujengNessuna valutazione finora
- Occipital LobesDocumento46 pagineOccipital LobesLakshya J Basumatary100% (1)
- October 2022 Complete Month CA English - CompressedDocumento117 pagineOctober 2022 Complete Month CA English - CompressedKing JNessuna valutazione finora
- Diagram Alir Dan Deskripsi Proses: Tugas 4Documento11 pagineDiagram Alir Dan Deskripsi Proses: Tugas 4FevitaNessuna valutazione finora
- Guidelines For Good Distribution Practices For Drugs, Cosmetics, Medical Devices and Household Chemical SubstancesDocumento4 pagineGuidelines For Good Distribution Practices For Drugs, Cosmetics, Medical Devices and Household Chemical SubstancessboaduappiahNessuna valutazione finora
- Report On Legal Medicine PowerpointDocumento31 pagineReport On Legal Medicine PowerpointEdwin VillaNessuna valutazione finora
- MalariaDocumento11 pagineMalariaWynli Fullo AncogNessuna valutazione finora