Potrebbero piacerti anche
- Valadi - Guillain-Barré SyndromeDocumento5 pagineValadi - Guillain-Barré SyndromeMarcelo BedoyaNessuna valutazione finora
- Ubogu - Inflammatory NeuropathiesDocumento24 pagineUbogu - Inflammatory NeuropathiesMarcelo BedoyaNessuna valutazione finora
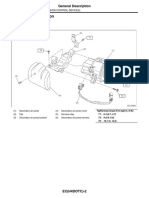
- Emission+Control+ (Aux +Emission+Control+Devices) + (H4DOTC)Documento27 pagineEmission+Control+ (Aux +Emission+Control+Devices) + (H4DOTC)Marcelo BedoyaNessuna valutazione finora
- Asbury - Assesment of Current Diagnostic Criteria For GBSDocumento4 pagineAsbury - Assesment of Current Diagnostic Criteria For GBSMarcelo BedoyaNessuna valutazione finora
- 2014 Fokke GBS Brighton Brain 2014Documento11 pagine2014 Fokke GBS Brighton Brain 2014Hikmat SatriaNessuna valutazione finora
- Pokemon: Opening Theme: XylophoneDocumento17 paginePokemon: Opening Theme: XylophoneMarcelo BedoyaNessuna valutazione finora
- +09 US Geological Survey - Mineral Commodity Summaries 2016Documento205 pagine+09 US Geological Survey - Mineral Commodity Summaries 2016Marcelo BedoyaNessuna valutazione finora
- 13 Patrick - Lead Toxicity - Exposure, Evaluation Adn TreatmentDocumento21 pagine13 Patrick - Lead Toxicity - Exposure, Evaluation Adn TreatmentMarcelo BedoyaNessuna valutazione finora
- CG54 MigratedDocumento34 pagineCG54 MigratedMarcelo BedoyaNessuna valutazione finora
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (895)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (400)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (588)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (74)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (345)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2259)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (121)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- Drug Mefenamic AcidDocumento2 pagineDrug Mefenamic AcidMarNessuna valutazione finora
- Edit 02 Eka, Wanty, Maya-PPT Konfrens 14 JuniDocumento29 pagineEdit 02 Eka, Wanty, Maya-PPT Konfrens 14 JuniMaya Rosmaria PNessuna valutazione finora
- Homeopathy Mother Tinctures Internal and External UseDocumento8 pagineHomeopathy Mother Tinctures Internal and External Useyogeshydd50% (2)
- RADS - USG Worksheet TI-RADSDocumento2 pagineRADS - USG Worksheet TI-RADSpriyaNessuna valutazione finora
- Pericarditis NCLEX Review: Serous Fluid Is Between The Parietal and Visceral LayerDocumento3 paginePericarditis NCLEX Review: Serous Fluid Is Between The Parietal and Visceral LayerJustine Dinice MunozNessuna valutazione finora
- Trichoscopic Diagnosis of Cutaneous Pelodera Strongyloides Infestation in A DogDocumento5 pagineTrichoscopic Diagnosis of Cutaneous Pelodera Strongyloides Infestation in A DogRebeka MenezesNessuna valutazione finora
- General - Pathology 2Documento15 pagineGeneral - Pathology 2ahmed jarad100% (2)
- 500 Nursing QuestionsDocumento209 pagine500 Nursing QuestionsFilipino Nurses Central90% (20)
- Seminar: DiagnosisDocumento14 pagineSeminar: DiagnosisyenyenNessuna valutazione finora
- Stroke: BackgroundDocumento10 pagineStroke: Backgroundjhay-r reyesNessuna valutazione finora
- COVID-19 Quiz Explanations - Coursera - Evernote Web PDFDocumento6 pagineCOVID-19 Quiz Explanations - Coursera - Evernote Web PDFvito0684Nessuna valutazione finora
- DSM V Clinical Cases - Chapter 12 Sleep Wake DisordersDocumento13 pagineDSM V Clinical Cases - Chapter 12 Sleep Wake DisordersIzzyinOzzieNessuna valutazione finora
- Respiratory PathologyDocumento62 pagineRespiratory PathologyErnest ReddcliffvcksuNessuna valutazione finora
- 1.endo PerioLesionPartIThePathogenesisDocumento8 pagine1.endo PerioLesionPartIThePathogenesisMaulida SyafarinaNessuna valutazione finora
- WCS 015 - Shortness of Breath in A Construction Site Worker - Occupational Lung Diseases - Pulmonary Fibrosis - Workman's Compensation by DR DCL LamDocumento60 pagineWCS 015 - Shortness of Breath in A Construction Site Worker - Occupational Lung Diseases - Pulmonary Fibrosis - Workman's Compensation by DR DCL LamJenniferFooNessuna valutazione finora
- Toksikologi: Vidi Ika Hastari Stikes Harapan Bangsa Jember 2020Documento167 pagineToksikologi: Vidi Ika Hastari Stikes Harapan Bangsa Jember 2020Akhmad.Arief.NofiantoNessuna valutazione finora
- Acute Fatty Liver With PregnancyDocumento50 pagineAcute Fatty Liver With PregnancyDr. mohammed100% (1)
- Antiamoebic & Other Antiprotozoal DrugsDocumento47 pagineAntiamoebic & Other Antiprotozoal DrugsAmit ShahNessuna valutazione finora
- Fluid and Electrolyte Balance: Presenter: Dr. Siyum Mathewos (Omfs-Ri) Modulator: Dr. Dereje (Omfs, Consultant)Documento87 pagineFluid and Electrolyte Balance: Presenter: Dr. Siyum Mathewos (Omfs-Ri) Modulator: Dr. Dereje (Omfs, Consultant)Siyum MathewosNessuna valutazione finora
- UntitledDocumento14 pagineUntitlednaresh kumarNessuna valutazione finora
- 7.saq Miscellaneous QuestionsDocumento554 pagine7.saq Miscellaneous QuestionsdoctorirfanNessuna valutazione finora
- Ineffectuve Breathign PatternDocumento2 pagineIneffectuve Breathign PatternDiana Marie Magango FranciaNessuna valutazione finora
- TB Guideline TreatmentDocumento14 pagineTB Guideline TreatmentNovii NoviiNessuna valutazione finora
- Brain InfectionDocumento61 pagineBrain Infectionmanisha paikarayNessuna valutazione finora
- Parkinson S DiseaseDocumento91 pagineParkinson S DiseaseTrisha Tolentino100% (1)
- Caparative and SuperllativeDocumento10 pagineCaparative and SuperllativeLiing RacNessuna valutazione finora
- Hypertrophic Pyloric StenosisDocumento17 pagineHypertrophic Pyloric StenosisMohammed Fareed100% (1)
- Cell Comparison ChartDocumento3 pagineCell Comparison ChartJake BryantNessuna valutazione finora
- Fungi: Galactomannan and 1,3-β - Glucan Testing for the Diagnosis of Invasive AspergillosisDocumento8 pagineFungi: Galactomannan and 1,3-β - Glucan Testing for the Diagnosis of Invasive AspergillosisntnquynhproNessuna valutazione finora
- Option D (Postductal Coarctation of The Aorta) Is CorrectDocumento50 pagineOption D (Postductal Coarctation of The Aorta) Is Correctanimebests9Nessuna valutazione finora