Potrebbero piacerti anche
- Colloidal Silver Medical Treatment RediscoveredDocumento4 pagineColloidal Silver Medical Treatment RediscoveredVince MiltonNessuna valutazione finora
- Colloidal Silver - Cs - DetailsDocumento28 pagineColloidal Silver - Cs - DetailsmobsivacNessuna valutazione finora
- Silver Sol Scientific ResearchDocumento3 pagineSilver Sol Scientific ResearchALKESWW100% (1)
- Silver in Wound TherapyDocumento28 pagineSilver in Wound TherapyGreg Wilby100% (1)
- Silver Nanoparticles: Mycogenesis, Characterization and Its Anti Plant Pathogenic ApplicationsDocumento10 pagineSilver Nanoparticles: Mycogenesis, Characterization and Its Anti Plant Pathogenic ApplicationsImpact JournalsNessuna valutazione finora
- Use of Coconut OilDocumento5 pagineUse of Coconut OilRakeshKumarNessuna valutazione finora
- Faraday's Law Lab Web VersionDocumento10 pagineFaraday's Law Lab Web Versionv9mpir5Nessuna valutazione finora
- Particle Size and Surface Area Are Important Parameters in The Development of A DrugDocumento8 pagineParticle Size and Surface Area Are Important Parameters in The Development of A Drugvicbart11Nessuna valutazione finora
- Proteins PDFDocumento20 pagineProteins PDFDOMADO EBTISHAMNessuna valutazione finora
- Development and Validation of A Miniature Programmable TDCS DeviceDocumento8 pagineDevelopment and Validation of A Miniature Programmable TDCS DevicenetoNessuna valutazione finora
- Adam1992 Hypochlorous Acid Decomposition in The PH 5-8 RegionDocumento8 pagineAdam1992 Hypochlorous Acid Decomposition in The PH 5-8 RegionGregorio ValeroNessuna valutazione finora
- Chlorination of Natural Waters: Hocl CL H 0 H CLDocumento5 pagineChlorination of Natural Waters: Hocl CL H 0 H CLmuratNessuna valutazione finora
- Thermodynamics of Ag CL H, O, Ag BR H, ODocumento9 pagineThermodynamics of Ag CL H, O, Ag BR H, Oहरिओम हरीNessuna valutazione finora
- AgDocumento9 pagineAgnureen92Nessuna valutazione finora
- Sample Meal Plan Low-Carb Diet TextDocumento2 pagineSample Meal Plan Low-Carb Diet TextJan FoxNessuna valutazione finora
- Neutrophils and Their DisordersDocumento41 pagineNeutrophils and Their DisordersGracekejiNessuna valutazione finora
- Control Relay Using IR SensorDocumento5 pagineControl Relay Using IR Sensorsmartxdigital marketNessuna valutazione finora
- Electrolysis Process ExplainedDocumento4 pagineElectrolysis Process ExplainedRiddhiSolankiNessuna valutazione finora
- Beck Protocol Newsletter Nov 02Documento4 pagineBeck Protocol Newsletter Nov 02inalight100% (1)
- Redox and DisinfectionDocumento41 pagineRedox and DisinfectionKanchanNessuna valutazione finora
- Ag BulletDocumento7 pagineAg BulletdevendrakphyNessuna valutazione finora
- Synthesis of Silver Nanoparticles by Using Sodium BorohydrideDocumento5 pagineSynthesis of Silver Nanoparticles by Using Sodium BorohydrideGil SalazarNessuna valutazione finora
- Colloidal Silver Fabrication Using The Spark Discharge System and PDFDocumento5 pagineColloidal Silver Fabrication Using The Spark Discharge System and PDFWilton Carlos SilvaNessuna valutazione finora
- Redox ReactionsDocumento8 pagineRedox ReactionsAbhayNessuna valutazione finora
- A Review On Electrochemical Technologies For Water DisinfectionDocumento18 pagineA Review On Electrochemical Technologies For Water DisinfectionArun Siddarth100% (3)
- Antibacterial Medicines Obtained by Using The Silver NanoparticlesDocumento3 pagineAntibacterial Medicines Obtained by Using The Silver NanoparticlesdropsyNessuna valutazione finora
- Silverreport PDFDocumento4 pagineSilverreport PDFCarlos ChaflaNessuna valutazione finora
- AgNP Silver - Nanoparticles - Synthesized - by - in - V 2 PDFDocumento13 pagineAgNP Silver - Nanoparticles - Synthesized - by - in - V 2 PDFyousra bibaNessuna valutazione finora
- Colloidal Silver A Simple Homemade RemedyDocumento9 pagineColloidal Silver A Simple Homemade RemedyGCarrington96Nessuna valutazione finora
- MEGASONICS IN FOOD PROCESSINGDocumento27 pagineMEGASONICS IN FOOD PROCESSINGJasmin OotyNessuna valutazione finora
- The Electrochemical Detection and Characterization of Silver Nanoparticles in Aqueous Solution PDFDocumento3 pagineThe Electrochemical Detection and Characterization of Silver Nanoparticles in Aqueous Solution PDFNayarik HerreraNessuna valutazione finora
- TDCS GerätDocumento18 pagineTDCS GerätPeter Benedikt WeberNessuna valutazione finora
- Eberhardt - Reactive Oxygen Metabolites-Chemistry and Medical ConsequencesDocumento609 pagineEberhardt - Reactive Oxygen Metabolites-Chemistry and Medical ConsequencesGirish Kishor PaiNessuna valutazione finora
- Purificación de Agua Con NanoparticulasDocumento91 paginePurificación de Agua Con NanoparticulaspedrojrsNessuna valutazione finora
- Application of Electrolyzed Water For Improving Pork Meat QualityDocumento7 pagineApplication of Electrolyzed Water For Improving Pork Meat QualityAnyelo MurilloNessuna valutazione finora
- Colloidal SilverDocumento4 pagineColloidal Silvermseagle100% (1)
- SILVER Nanoparticles PDFDocumento342 pagineSILVER Nanoparticles PDFFERNANDO JOSE NOVAESNessuna valutazione finora
- Production of Colloidal SilverDocumento10 pagineProduction of Colloidal SilverjwalterlimaNessuna valutazione finora
- The Silver Edge CatalogueDocumento8 pagineThe Silver Edge CatalogueDino RubioNessuna valutazione finora
- Galvanic CurrentDocumento26 pagineGalvanic CurrentRana M ArslanNessuna valutazione finora
- Microbial Production of NanoparticlesDocumento11 pagineMicrobial Production of NanoparticlesnadiafarhanaNessuna valutazione finora
- 26 Ways To Use Silver SolDocumento8 pagine26 Ways To Use Silver SolALKESWWNessuna valutazione finora
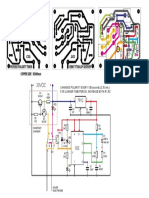
- Peverse Polarity Timer CSG: CHANGES POLARITY EVERY 130 Seconds (2,10 Min.) For Longer Time Period, Increase Both R1, R2Documento1 paginaPeverse Polarity Timer CSG: CHANGES POLARITY EVERY 130 Seconds (2,10 Min.) For Longer Time Period, Increase Both R1, R2Carlos ChaflaNessuna valutazione finora
- Making A Colloidal Silver GeneratorDocumento5 pagineMaking A Colloidal Silver Generatorsanyu33333Nessuna valutazione finora
- Circuit ElectrinicDocumento2 pagineCircuit ElectrinicfamtaluNessuna valutazione finora
- AgPURE TDSDocumento10 pagineAgPURE TDStomellefsenNessuna valutazione finora
- LM317L 3-Terminal Adjustable Regulator: FeaturesDocumento25 pagineLM317L 3-Terminal Adjustable Regulator: FeaturespaulpuscasuNessuna valutazione finora
- Relay Basics and DIYDocumento6 pagineRelay Basics and DIYJunior ElimeelogodavejuniorNessuna valutazione finora
- CS Marvin RobeyDocumento7 pagineCS Marvin RobeySandra HarrisNessuna valutazione finora
- Plan 8 CS Generator PDFDocumento3 paginePlan 8 CS Generator PDFWansys UnoNessuna valutazione finora
- Sibbald RG Et All, 2011Documento6 pagineSibbald RG Et All, 2011safiraNessuna valutazione finora
- Building A Perf-Board Defib TesterDocumento7 pagineBuilding A Perf-Board Defib TesterElectrónica BiomédicaNessuna valutazione finora
- Silver-Based Polymeric Nanocomposites As Antimicrobial Coatings For Biomedical ApplicationsDocumento57 pagineSilver-Based Polymeric Nanocomposites As Antimicrobial Coatings For Biomedical ApplicationsDimas PradhasumitraNessuna valutazione finora
- Usb Powered Colloidal Silver GeneratorDocumento14 pagineUsb Powered Colloidal Silver GeneratorVíctor Faucheret100% (1)
- SilverMAX Instruction Manual for Colloidal Silver GeneratorDocumento3 pagineSilverMAX Instruction Manual for Colloidal Silver GeneratorLiviu AngelescuNessuna valutazione finora
- Silver: A Versatile and Valuable MetalDocumento11 pagineSilver: A Versatile and Valuable MetalSP C100% (1)
- Electro Merge??Documento621 pagineElectro Merge??Sadaf MasoodNessuna valutazione finora
- 6 Facts About Colloidal Silver For BeginnersDocumento2 pagine6 Facts About Colloidal Silver For BeginnersduhitijeloNessuna valutazione finora
- People of The LieDocumento7 paginePeople of The LieNatasha Myers0% (2)
- Colloidal Silver - Dr. Robert BeckerDocumento2 pagineColloidal Silver - Dr. Robert Beckerjuanitos111100% (1)
- Americas Frontline DoctorsDocumento3 pagineAmericas Frontline DoctorsNwoinfowarrior KilluminatiNessuna valutazione finora
- 2020 01 30 927871v1 FullDocumento14 pagine2020 01 30 927871v1 FullJohn Roberts100% (1)
- V.ivanov - Financing Opportunities and ChallengesDocumento19 pagineV.ivanov - Financing Opportunities and ChallengesNwoinfowarrior KilluminatiNessuna valutazione finora
- 2014 ARSOF Operating Concept 2022 U.S. Special Operations CommandDocumento68 pagine2014 ARSOF Operating Concept 2022 U.S. Special Operations CommandNwoinfowarrior KilluminatiNessuna valutazione finora
- CORVELVA Study On The Chemical Composition Profile of Infanrix HexaDocumento11 pagineCORVELVA Study On The Chemical Composition Profile of Infanrix HexaNwoinfowarrior KilluminatiNessuna valutazione finora
- Air Force Research Laboratory in Vitro Toxicity of Aluminum Nanoparticles in Rat Alveolar MacrophagesDocumento10 pagineAir Force Research Laboratory in Vitro Toxicity of Aluminum Nanoparticles in Rat Alveolar MacrophagesNwoinfowarrior KilluminatiNessuna valutazione finora
- 140554NCJRS PDFDocumento49 pagine140554NCJRS PDFtravis smith100% (1)
- Vaxxed Unvaxxed Full Presentation Parts I VIDocumento42 pagineVaxxed Unvaxxed Full Presentation Parts I VINwoinfowarrior KilluminatiNessuna valutazione finora
- Crying Wolf - Laird WilcoxDocumento112 pagineCrying Wolf - Laird WilcoxadavielchiùNessuna valutazione finora
- Document PDFDocumento55 pagineDocument PDFNwoinfowarrior KilluminatiNessuna valutazione finora
- The Chemistry in ContrailsDocumento111 pagineThe Chemistry in ContrailsNwoinfowarrior KilluminatiNessuna valutazione finora
- Affidavit of Truth Template #1 #TeamTylerDocumento6 pagineAffidavit of Truth Template #1 #TeamTylerNwoinfowarrior Killuminati100% (16)
- Take Back Your PowerDocumento42 pagineTake Back Your Poweranon-51752295% (21)
- 2014 ARSOF Operating Concept 2022 Part 2 - U.S. Special Operations CommandDocumento32 pagine2014 ARSOF Operating Concept 2022 Part 2 - U.S. Special Operations CommandNwoinfowarrior Killuminati100% (1)
- Otb 121109 8 November 2012 Treason Complaint AdministrationDocumento1 paginaOtb 121109 8 November 2012 Treason Complaint AdministrationCensored News NowNessuna valutazione finora
- FEMA Homeland Security Exercise and Evaluation Program (HSEEP) Actor Waiver FormDocumento1 paginaFEMA Homeland Security Exercise and Evaluation Program (HSEEP) Actor Waiver FormNwoinfowarrior KilluminatiNessuna valutazione finora
- Otb 121109 8 November 2012 Formal Criminal Complaint Obama TreasonDocumento4 pagineOtb 121109 8 November 2012 Formal Criminal Complaint Obama TreasonCensored News NowNessuna valutazione finora
- Benghazi Interim Progress ReportDocumento46 pagineBenghazi Interim Progress ReportPRMurphyNessuna valutazione finora
- 1974 Kissinger Memo 200Documento2 pagine1974 Kissinger Memo 200Nwoinfowarrior KilluminatiNessuna valutazione finora
- Lucija Tomljenovic - The Vaccination Policy and The Code of Practice of The JCVIDocumento45 pagineLucija Tomljenovic - The Vaccination Policy and The Code of Practice of The JCVITratincica StewartNessuna valutazione finora
- Obama Cloning & The Coming Space WarDocumento7 pagineObama Cloning & The Coming Space WarNwoinfowarrior Killuminati100% (1)
- HAMP ChemtrailsDocumento15 pagineHAMP ChemtrailsNwoinfowarrior KilluminatiNessuna valutazione finora
- Marijuana Poll - Pot Smokers Outnumber Prohibitionists in California PollDocumento6 pagineMarijuana Poll - Pot Smokers Outnumber Prohibitionists in California PollNwoinfowarrior KilluminatiNessuna valutazione finora
- Epperson - The Unseen Hand - An Introduction To The Conspiratorial View of History (1994)Documento476 pagineEpperson - The Unseen Hand - An Introduction To The Conspiratorial View of History (1994)oihf99% (68)
- A Brief Primer On Colloidal SilverDocumento4 pagineA Brief Primer On Colloidal SilverNwoinfowarrior KilluminatiNessuna valutazione finora
- The Obama Deception BilbliographyDocumento31 pagineThe Obama Deception BilbliographyMattNessuna valutazione finora
- Chemtrail PDFDocumento128 pagineChemtrail PDFsandmtn67% (6)
- Brief History of Colloidal SilverDocumento3 pagineBrief History of Colloidal SilverNwoinfowarrior KilluminatiNessuna valutazione finora
- Privacy Lawsuit Targets Net Giants (Scribd) Over Zombie' CookiesDocumento126 paginePrivacy Lawsuit Targets Net Giants (Scribd) Over Zombie' CookiesNwoinfowarrior KilluminatiNessuna valutazione finora
- Bilderberg Meetings BrochureDocumento38 pagineBilderberg Meetings BrochureNwoinfowarrior Killuminati100% (1)
- Carbapenem Resistant Enterobacteriaceae - StatPearls - NCBI BookshelfDocumento9 pagineCarbapenem Resistant Enterobacteriaceae - StatPearls - NCBI BookshelfOG3 PolizuNessuna valutazione finora
- Conversion MG - DL To Mmol - LDocumento6 pagineConversion MG - DL To Mmol - LshrinivastNessuna valutazione finora
- Tata Laksana PneumoniaDocumento29 pagineTata Laksana PneumoniaSRI WIDOWATINessuna valutazione finora
- Lecture 13 Tumor ImmunologyDocumento99 pagineLecture 13 Tumor Immunologyمحمود محمد100% (1)
- Measles Basics CDCDocumento2 pagineMeasles Basics CDCStephen LoiaconiNessuna valutazione finora
- Biology Unit 4 Long AnswersDocumento3 pagineBiology Unit 4 Long Answersbad123wolf101_614598100% (1)
- Resistance To White Rot Disease and Enhancement of Yield and Its Components by Selection in Mutants of Two Garlic CultivarsDocumento13 pagineResistance To White Rot Disease and Enhancement of Yield and Its Components by Selection in Mutants of Two Garlic CultivarsShailendra RajanNessuna valutazione finora
- Pi Is 0161642015004194Documento8 paginePi Is 0161642015004194debbyNessuna valutazione finora
- Microorganisms 09 00136 v2Documento19 pagineMicroorganisms 09 00136 v2elalaoui25Nessuna valutazione finora
- Frequency ChartDocumento12 pagineFrequency ChartGeorgina ĐukićNessuna valutazione finora
- Xam Idea Biology - Class 12 Term 1 and 2 Question BankDocumento587 pagineXam Idea Biology - Class 12 Term 1 and 2 Question BankAnmol Beniwal79% (29)
- Hematopoiesis Reading NotesDocumento7 pagineHematopoiesis Reading NotesMemeowwNessuna valutazione finora
- Understanding Genitourinary System CytologyDocumento130 pagineUnderstanding Genitourinary System Cytologyaaes2Nessuna valutazione finora
- PenisDocumento23 paginePenisWira DharmaNessuna valutazione finora
- Chap 16 Part 2 Major Arms of The Immune System Humoral Immunity (Antibodies)Documento5 pagineChap 16 Part 2 Major Arms of The Immune System Humoral Immunity (Antibodies)clrssNessuna valutazione finora
- Booklet 2018Documento34 pagineBooklet 2018BaluErnestoNessuna valutazione finora
- Introduction To VirologyDocumento22 pagineIntroduction To VirologymicroperadeniyaNessuna valutazione finora
- Ebola - Class 12 Biology Investigatory ProjectDocumento15 pagineEbola - Class 12 Biology Investigatory ProjectSourav Panda60% (5)
- Clippers and Its MimicsDocumento12 pagineClippers and Its Mimicsveerraju tvNessuna valutazione finora
- N"SF) VF) K Nufpg) DoDocumento4 pagineN"SF) VF) K Nufpg) DoRajesh KoiralaNessuna valutazione finora
- Dapus MakalahDocumento2 pagineDapus MakalahAndra NurjayaNessuna valutazione finora
- Lesson#2 - Non Mendelian Patterns of InheritanceDocumento11 pagineLesson#2 - Non Mendelian Patterns of Inheritancejerikbenito46Nessuna valutazione finora
- Literature Review of Cervix CancerDocumento6 pagineLiterature Review of Cervix Cancerzyfepyfej0p2100% (1)
- Karen-Shaul 2017 Cell PDFDocumento33 pagineKaren-Shaul 2017 Cell PDFVirgínia Chaves de LimaNessuna valutazione finora
- Microbiolspec - Arba 0009 2017Documento26 pagineMicrobiolspec - Arba 0009 2017Rossio Noelia Jurado NaciónNessuna valutazione finora
- Protozoan Fecal SmearDocumento17 pagineProtozoan Fecal SmearLeigh Ann TanpoNessuna valutazione finora
- The Role of Nurses in Providing Sex Education for HIV/AIDS PatientsDocumento15 pagineThe Role of Nurses in Providing Sex Education for HIV/AIDS PatientsXHavierNessuna valutazione finora
- COVID-19 - A Study PDFDocumento4 pagineCOVID-19 - A Study PDFInternational Journal of Innovative Science and Research TechnologyNessuna valutazione finora
- Gabatilla Genbio q3m1-18Documento23 pagineGabatilla Genbio q3m1-18GABATILLA JAN RYLNessuna valutazione finora
- C19 - Haemophilus and Other Fastidious Gram-Negative BacilliDocumento19 pagineC19 - Haemophilus and Other Fastidious Gram-Negative BacilliJezzah Mae CañeteNessuna valutazione finora
- Uncontrolled Spread: Why COVID-19 Crushed Us and How We Can Defeat the Next PandemicDa EverandUncontrolled Spread: Why COVID-19 Crushed Us and How We Can Defeat the Next PandemicNessuna valutazione finora
- Deaths of Despair and the Future of CapitalismDa EverandDeaths of Despair and the Future of CapitalismValutazione: 4.5 su 5 stelle4.5/5 (30)
- The Atlas of Disease: Mapping Deadly Epidemics and Contagion from the Plague to the CoronavirusDa EverandThe Atlas of Disease: Mapping Deadly Epidemics and Contagion from the Plague to the CoronavirusValutazione: 4.5 su 5 stelle4.5/5 (10)
- Epic Measures: One Doctor. Seven Billion Patients.Da EverandEpic Measures: One Doctor. Seven Billion Patients.Valutazione: 4 su 5 stelle4/5 (13)
- Summary: The Myth of Normal: Trauma, Illness, and Healing in a Toxic Culture By Gabor Maté MD & Daniel Maté: Key Takeaways, Summary & AnalysisDa EverandSummary: The Myth of Normal: Trauma, Illness, and Healing in a Toxic Culture By Gabor Maté MD & Daniel Maté: Key Takeaways, Summary & AnalysisValutazione: 4 su 5 stelle4/5 (9)
- Do You Believe in Magic?: The Sense and Nonsense of Alternative MedicineDa EverandDo You Believe in Magic?: The Sense and Nonsense of Alternative MedicineNessuna valutazione finora
- The Wisdom of Plagues: Lessons from 25 Years of Covering PandemicsDa EverandThe Wisdom of Plagues: Lessons from 25 Years of Covering PandemicsValutazione: 4.5 su 5 stelle4.5/5 (5)
- Nutritional and Therapeutic Interventions for Diabetes and Metabolic SyndromeDa EverandNutritional and Therapeutic Interventions for Diabetes and Metabolic SyndromeNessuna valutazione finora
- Epidemics and Society: From the Black Death to the PresentDa EverandEpidemics and Society: From the Black Death to the PresentValutazione: 4.5 su 5 stelle4.5/5 (9)
- Clean: Overcoming Addiction and Ending America’s Greatest TragedyDa EverandClean: Overcoming Addiction and Ending America’s Greatest TragedyValutazione: 4 su 5 stelle4/5 (18)
- The HPV Vaccine On Trial: Seeking Justice For A Generation BetrayedDa EverandThe HPV Vaccine On Trial: Seeking Justice For A Generation BetrayedValutazione: 4.5 su 5 stelle4.5/5 (13)
- The Nocebo Effect: When Words Make You SickDa EverandThe Nocebo Effect: When Words Make You SickNessuna valutazione finora
- Understanding Addiction: Know Science, No StigmaDa EverandUnderstanding Addiction: Know Science, No StigmaNessuna valutazione finora
- The Bodies of Others: The New Authoritarians, COVID-19 and The War Against the HumanDa EverandThe Bodies of Others: The New Authoritarians, COVID-19 and The War Against the HumanValutazione: 4.5 su 5 stelle4.5/5 (12)
- The Truth about Wuhan: How I Uncovered the Biggest Lie in HistoryDa EverandThe Truth about Wuhan: How I Uncovered the Biggest Lie in HistoryValutazione: 4 su 5 stelle4/5 (6)
- Quick Fixes: Drugs in America from Prohibition to the 21st Century BingeDa EverandQuick Fixes: Drugs in America from Prohibition to the 21st Century BingeNessuna valutazione finora
- The Transformation: Discovering Wholeness and Healing After TraumaDa EverandThe Transformation: Discovering Wholeness and Healing After TraumaValutazione: 4 su 5 stelle4/5 (70)
- There Are No Accidents: The Deadly Rise of Injury and Disaster—Who Profits and Who Pays the PriceDa EverandThere Are No Accidents: The Deadly Rise of Injury and Disaster—Who Profits and Who Pays the PriceValutazione: 4.5 su 5 stelle4.5/5 (15)
- Microbiological Quality of FoodsDa EverandMicrobiological Quality of FoodsL SlanetzNessuna valutazione finora
- The Gut-Immune Connection: How Understanding the Connection Between Food and Immunity Can Help Us Regain Our HealthDa EverandThe Gut-Immune Connection: How Understanding the Connection Between Food and Immunity Can Help Us Regain Our HealthNessuna valutazione finora
- Blood Runs Coal: The Yablonski Murders and the Battle for the United Mine Workers of AmericaDa EverandBlood Runs Coal: The Yablonski Murders and the Battle for the United Mine Workers of AmericaValutazione: 4.5 su 5 stelle4.5/5 (2)
- A Good Time to Be Born: How Science and Public Health Gave Children a FutureDa EverandA Good Time to Be Born: How Science and Public Health Gave Children a FutureValutazione: 5 su 5 stelle5/5 (1)
- The War on Informed Consent: The Persecution of Dr. Paul Thomas by the Oregon Medical BoardDa EverandThe War on Informed Consent: The Persecution of Dr. Paul Thomas by the Oregon Medical BoardValutazione: 3 su 5 stelle3/5 (2)
- Arthritis Diet: Anti-inflammatory Diet for Arthritis Pain ReliefDa EverandArthritis Diet: Anti-inflammatory Diet for Arthritis Pain ReliefNessuna valutazione finora
- War on Ivermectin: The Medicine that Saved Millions and Could Have Ended the PandemicDa EverandWar on Ivermectin: The Medicine that Saved Millions and Could Have Ended the PandemicValutazione: 4 su 5 stelle4/5 (7)
- Doctored: The Disillusionment of an American PhysicianDa EverandDoctored: The Disillusionment of an American PhysicianValutazione: 4 su 5 stelle4/5 (11)