Potrebbero piacerti anche
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- FallsintheElderly PDFDocumento12 pagineFallsintheElderly PDFNa d'Nazaie CodeNessuna valutazione finora
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (895)
- FallsintheElderly PDFDocumento12 pagineFallsintheElderly PDFNa d'Nazaie CodeNessuna valutazione finora
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5794)
- Enhancing Nurses Pain Assessment To Improve.11Documento2 pagineEnhancing Nurses Pain Assessment To Improve.11Na d'Nazaie CodeNessuna valutazione finora
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (399)
- NIH Public Access: Interventions To Improve Walking in Older AdultsDocumento13 pagineNIH Public Access: Interventions To Improve Walking in Older AdultsNa d'Nazaie CodeNessuna valutazione finora
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (266)
- FASP Fetal Anomaly Ultrasound Screening Pathwayv12Documento1 paginaFASP Fetal Anomaly Ultrasound Screening Pathwayv12Na d'Nazaie CodeNessuna valutazione finora
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- Model Klasifikasi Menggunakan Metode Regresi Logistik Dan Multivariate Adaptive Regression Splines (Mars) (Studi Kasus: Data Survei Biaya Hidup (SBH) Kota Kediri Tahun 2012)Documento12 pagineModel Klasifikasi Menggunakan Metode Regresi Logistik Dan Multivariate Adaptive Regression Splines (Mars) (Studi Kasus: Data Survei Biaya Hidup (SBH) Kota Kediri Tahun 2012)Na d'Nazaie CodeNessuna valutazione finora
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
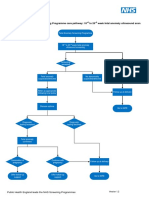
- FASPDownsT21EdwardsT18andPatausT13pathway11 PDFDocumento1 paginaFASPDownsT21EdwardsT18andPatausT13pathway11 PDFNa d'Nazaie CodeNessuna valutazione finora
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- 2 10 1 PBDocumento3 pagine2 10 1 PBNa d'Nazaie CodeNessuna valutazione finora
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (588)
- R1 - Vo3No4 KJHDocumento14 pagineR1 - Vo3No4 KJHNa d'Nazaie CodeNessuna valutazione finora
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- Kualitas HidupDocumento8 pagineKualitas Hidupsrihandayani1984Nessuna valutazione finora
- Rita Dwi HartantiDocumento9 pagineRita Dwi HartantiNa d'Nazaie CodeNessuna valutazione finora
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- Kusiima Chs Masters Abstract PDFDocumento3 pagineKusiima Chs Masters Abstract PDFNa d'Nazaie CodeNessuna valutazione finora
- ITS Undergraduate 18940 Bibliographypdf PDFDocumento2 pagineITS Undergraduate 18940 Bibliographypdf PDFNa d'Nazaie CodeNessuna valutazione finora
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2259)
- Ipi200729 PDFDocumento14 pagineIpi200729 PDFNa d'Nazaie CodeNessuna valutazione finora
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (73)
- Calculating The Sample Size of Multivariate Populations: Norms of RepresentationDocumento6 pagineCalculating The Sample Size of Multivariate Populations: Norms of RepresentationNa d'Nazaie CodeNessuna valutazione finora
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (344)
- WOQOL Measuring QV MentalDocumento15 pagineWOQOL Measuring QV MentalpenfoNessuna valutazione finora
- McCallum (2001) Sample Size in Factor Analysis The Role of Model ErrorDocumento27 pagineMcCallum (2001) Sample Size in Factor Analysis The Role of Model ErrorNa d'Nazaie CodeNessuna valutazione finora
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- Dochtermann Jenkins ResponseDocumento11 pagineDochtermann Jenkins ResponseNa d'Nazaie CodeNessuna valutazione finora
- Circulation 2014 Hansen 1859 67Documento15 pagineCirculation 2014 Hansen 1859 67Na d'Nazaie CodeNessuna valutazione finora
- JurnalDocumento87 pagineJurnalNa d'Nazaie CodeNessuna valutazione finora
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- Power and Minimal Sample Size For Multivariate Analysis of MicroarraysDocumento1 paginaPower and Minimal Sample Size For Multivariate Analysis of MicroarraysNa d'Nazaie CodeNessuna valutazione finora
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- 20Documento3 pagine20Na d'Nazaie CodeNessuna valutazione finora
- Circulation 2014 Hansen 1859 67Documento15 pagineCirculation 2014 Hansen 1859 67Na d'Nazaie CodeNessuna valutazione finora
- Kuesioner SSQDocumento15 pagineKuesioner SSQNa d'Nazaie Code100% (3)
- Toxicon: SciencedirectDocumento14 pagineToxicon: SciencedirectNa d'Nazaie CodeNessuna valutazione finora
- The Blind MotherDocumento2 pagineThe Blind MotherNa d'Nazaie CodeNessuna valutazione finora
- 995 FullDocumento8 pagine995 FullNa d'Nazaie CodeNessuna valutazione finora
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (121)
- Circulation 2011 Kilgannon 2717 22Documento7 pagineCirculation 2011 Kilgannon 2717 22Na d'Nazaie CodeNessuna valutazione finora
- 1st Panel Inventory September 2021mdsDocumento199 pagine1st Panel Inventory September 2021mds김에렌Nessuna valutazione finora
- List of Meds Lot 6Documento2 pagineList of Meds Lot 6Joseph DavidNessuna valutazione finora
- The Concepts of Community Environmental HealthDocumento2 pagineThe Concepts of Community Environmental HealthJM Ramirez100% (1)
- Daftar Obat FarmasiDocumento26 pagineDaftar Obat FarmasiNoor KevNessuna valutazione finora
- SDG Legal Guide - Chapter 3 - V2Documento36 pagineSDG Legal Guide - Chapter 3 - V2Ahmed AbbasNessuna valutazione finora
- Dokumen - Tips - Daftar Obat KlinikDocumento9 pagineDokumen - Tips - Daftar Obat KlinikIke Annisa YuwelzaNessuna valutazione finora
- National Report - Blood Banks Data Collection 2016 PDFDocumento63 pagineNational Report - Blood Banks Data Collection 2016 PDFAnonymous xlXGhNWNessuna valutazione finora
- Gabriel Dec 22Documento146 pagineGabriel Dec 22Elsa ChristinaNessuna valutazione finora
- CV MustafaDocumento8 pagineCV MustafaMuna HassaneinNessuna valutazione finora
- Who FCH Cah 00.1Documento175 pagineWho FCH Cah 00.1Regita AyuNessuna valutazione finora
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- Nama Obat Jumlah Jenis Harga: Estimasi Persiapan Obat Kegiatan PramukaDocumento2 pagineNama Obat Jumlah Jenis Harga: Estimasi Persiapan Obat Kegiatan PramukaMiracle AcleNessuna valutazione finora
- Effectiveness of Self DefenceDocumento127 pagineEffectiveness of Self DefenceSAJIDA SHAIKHNessuna valutazione finora
- The Prevalence of Maternal Near Miss: A Systematic ReviewDocumento9 pagineThe Prevalence of Maternal Near Miss: A Systematic ReviewringgoNessuna valutazione finora
- Contoh Daftar Belanja Obat Praktek PribadiDocumento10 pagineContoh Daftar Belanja Obat Praktek PribadimeryNessuna valutazione finora
- University of Cebu - BaniladDocumento3 pagineUniversity of Cebu - BaniladKhylamarie VillalunaNessuna valutazione finora
- Pedia NotesDocumento3 paginePedia NotesNikki DiocampoNessuna valutazione finora
- 27 Juli 22 LKDocumento144 pagine27 Juli 22 LKhasib unigaNessuna valutazione finora
- Daftar Harga 13 Agustus 2022Documento27 pagineDaftar Harga 13 Agustus 2022Dhamar SetiaNessuna valutazione finora
- COVID-19: How and When Covid-19 StartedDocumento3 pagineCOVID-19: How and When Covid-19 StartedAhtesham AliNessuna valutazione finora
- Brazil: The Mais Médicos ProgrammeDocumento16 pagineBrazil: The Mais Médicos ProgrammeAhmad YaseenNessuna valutazione finora
- Update Stok FMM - MaretDocumento34 pagineUpdate Stok FMM - MaretErna RujuNessuna valutazione finora
- Rekap Lap Penunjang Medis 020121Documento2.611 pagineRekap Lap Penunjang Medis 020121hefikurniasariNessuna valutazione finora
- Okuda-Time Series Analysis of Under-Five MortalityDocumento61 pagineOkuda-Time Series Analysis of Under-Five MortalityBoniface Okuda100% (4)
- Reading ComprehensionDocumento32 pagineReading ComprehensionTofik MohammedNessuna valutazione finora
- Generic Drug ListDocumento4 pagineGeneric Drug Listapi-3711312Nessuna valutazione finora
- Anta Assignment SAMPLEDocumento3 pagineAnta Assignment SAMPLEMSKCNessuna valutazione finora
- 346 RLSLDocumento19 pagine346 RLSLparlindunganNessuna valutazione finora
- Pricelist Reguler 2019 PDFDocumento38 paginePricelist Reguler 2019 PDFAsri Adyttia SparKyuNessuna valutazione finora
- Laporan Obat HarianDocumento8 pagineLaporan Obat HarianNi Dar100% (1)
- ProdukDocumento36 pagineProdukazka gaming ytNessuna valutazione finora
- Uncontrolled Spread: Why COVID-19 Crushed Us and How We Can Defeat the Next PandemicDa EverandUncontrolled Spread: Why COVID-19 Crushed Us and How We Can Defeat the Next PandemicNessuna valutazione finora
- The Wisdom of Plagues: Lessons from 25 Years of Covering PandemicsDa EverandThe Wisdom of Plagues: Lessons from 25 Years of Covering PandemicsValutazione: 4.5 su 5 stelle4.5/5 (6)
- Deaths of Despair and the Future of CapitalismDa EverandDeaths of Despair and the Future of CapitalismValutazione: 4.5 su 5 stelle4.5/5 (30)
- The Gut-Immune Connection: How Understanding the Connection Between Food and Immunity Can Help Us Regain Our HealthDa EverandThe Gut-Immune Connection: How Understanding the Connection Between Food and Immunity Can Help Us Regain Our HealthNessuna valutazione finora
- Summary: The Myth of Normal: Trauma, Illness, and Healing in a Toxic Culture By Gabor Maté MD & Daniel Maté: Key Takeaways, Summary & AnalysisDa EverandSummary: The Myth of Normal: Trauma, Illness, and Healing in a Toxic Culture By Gabor Maté MD & Daniel Maté: Key Takeaways, Summary & AnalysisValutazione: 4 su 5 stelle4/5 (9)
- Do You Believe in Magic?: The Sense and Nonsense of Alternative MedicineDa EverandDo You Believe in Magic?: The Sense and Nonsense of Alternative MedicineNessuna valutazione finora
- There Are No Accidents: The Deadly Rise of Injury and Disaster—Who Profits and Who Pays the PriceDa EverandThere Are No Accidents: The Deadly Rise of Injury and Disaster—Who Profits and Who Pays the PriceValutazione: 4.5 su 5 stelle4.5/5 (11)