Potrebbero piacerti anche
- Singh 2011Documento84 pagineSingh 2011Iuliana NitaNessuna valutazione finora
- PRISMA P ChecklistDocumento2 paginePRISMA P ChecklistAssem GamalNessuna valutazione finora
- Boards' Fodder: AlopeciaDocumento2 pagineBoards' Fodder: AlopeciaIuliana NitaNessuna valutazione finora
- BMJ g7647 FullDocumento25 pagineBMJ g7647 FullIuliana NitaNessuna valutazione finora
- Therapeutic Monoclonal Antibodies and The Need For Targeted Pharmacovigilance in IndiaDocumento5 pagineTherapeutic Monoclonal Antibodies and The Need For Targeted Pharmacovigilance in IndiaIuliana NitaNessuna valutazione finora
- Extended Report: ObjectivesDocumento8 pagineExtended Report: ObjectivesIuliana NitaNessuna valutazione finora
- Mabs0401 0110Documento10 pagineMabs0401 0110Iuliana NitaNessuna valutazione finora
- Trends in Sunscreen Recommendation Among US Physicians: Original InvestigationDocumento5 pagineTrends in Sunscreen Recommendation Among US Physicians: Original InvestigationIuliana NitaNessuna valutazione finora
- SwichDocumento6 pagineSwichIuliana NitaNessuna valutazione finora
- Mabs0401 0110Documento10 pagineMabs0401 0110Iuliana NitaNessuna valutazione finora
- Stevenson 2017Documento13 pagineStevenson 2017Iuliana NitaNessuna valutazione finora
- Guidelines of Care For The Management of Acne VulgarisDocumento53 pagineGuidelines of Care For The Management of Acne VulgarisIuliana NitaNessuna valutazione finora
- Kew 442Documento9 pagineKew 442Iuliana NitaNessuna valutazione finora
- Stevenson 2017Documento13 pagineStevenson 2017Iuliana NitaNessuna valutazione finora
- Factors in Uencing The Immunogenicity of Therapeutic ProteinsDocumento7 pagineFactors in Uencing The Immunogenicity of Therapeutic ProteinsIuliana NitaNessuna valutazione finora
- ICMJE Form PDFDocumento1 paginaICMJE Form PDFsanjayb1008491Nessuna valutazione finora
- Am18 Poster Exhibits GuidelinesDocumento3 pagineAm18 Poster Exhibits GuidelinesIuliana NitaNessuna valutazione finora
- 2.1.2 - PRISMA 2009 ChecklistDocumento2 pagine2.1.2 - PRISMA 2009 ChecklistFiŗåš ÀßßâşNessuna valutazione finora
- Icmje Recommendations PDFDocumento17 pagineIcmje Recommendations PDFFebyan AbotNessuna valutazione finora
- On Diagnostic Rationality: Bad News, Good News, and The Symptom ResidueDocumento37 pagineOn Diagnostic Rationality: Bad News, Good News, and The Symptom ResidueIuliana NitaNessuna valutazione finora
- Jcad 10 3 s1 8Documento8 pagineJcad 10 3 s1 8Iuliana NitaNessuna valutazione finora
- How To Get PublishedDocumento2 pagineHow To Get PublishedIuliana NitaNessuna valutazione finora
- Doyle 2013Documento12 pagineDoyle 2013Iuliana NitaNessuna valutazione finora
- The Salford Psoriasis Index An Holistic Measure of Psoriasis SeverityDocumento5 pagineThe Salford Psoriasis Index An Holistic Measure of Psoriasis SeverityIuliana NitaNessuna valutazione finora
- Patient CommunicationDocumento16 paginePatient CommunicationIuliana NitaNessuna valutazione finora
- Communication and Active ListeningDocumento18 pagineCommunication and Active ListeningIuliana NitaNessuna valutazione finora
- EpilareDocumento10 pagineEpilareIuliana NitaNessuna valutazione finora
- Ultrasound Study of Entheses in Psoriasis Patients With or Without Musculoskeletal Symptoms A Prospective StudyDocumento5 pagineUltrasound Study of Entheses in Psoriasis Patients With or Without Musculoskeletal Symptoms A Prospective StudyIuliana NitaNessuna valutazione finora
- The Relationship Between Nail - and Distal Phalangeal BoneDocumento3 pagineThe Relationship Between Nail - and Distal Phalangeal BoneIuliana NitaNessuna valutazione finora
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5794)
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (895)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (400)
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (588)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (74)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (344)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (121)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- 95-03097 Ballvlv300350 WCB PDFDocumento26 pagine95-03097 Ballvlv300350 WCB PDFasitdeyNessuna valutazione finora
- CandyDocumento24 pagineCandySjdb FjfbNessuna valutazione finora
- Cln4u Task Prisons RubricsDocumento2 pagineCln4u Task Prisons RubricsJordiBdMNessuna valutazione finora
- Art Appreciation Chapter 3 SummaryDocumento6 pagineArt Appreciation Chapter 3 SummaryDiego A. Odchimar IIINessuna valutazione finora
- DHA - Jebel Ali Emergency Centre + RevisedDocumento5 pagineDHA - Jebel Ali Emergency Centre + RevisedJam EsNessuna valutazione finora
- The One With The ThumbDocumento4 pagineThe One With The Thumbnoelia20_09Nessuna valutazione finora
- BarricadeDocumento6 pagineBarricadeJithu PappachanNessuna valutazione finora
- OBOE GougerDocumento2 pagineOBOE GougerCarlos GaldámezNessuna valutazione finora
- Acute Suppurative Otitis MediaDocumento41 pagineAcute Suppurative Otitis Mediarani suwadjiNessuna valutazione finora
- Reference GuideDocumento88 pagineReference GuideAnonymous Qm0zbNk100% (1)
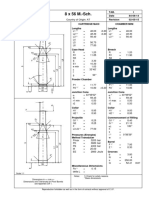
- 8 X 56 M.-SCH.: Country of Origin: ATDocumento1 pagina8 X 56 M.-SCH.: Country of Origin: ATMohammed SirelkhatimNessuna valutazione finora
- Investigation Data FormDocumento1 paginaInvestigation Data Formnildin danaNessuna valutazione finora
- This Is A Short Presentation To Explain The Character of Uncle Sam, Made by Ivo BogoevskiDocumento7 pagineThis Is A Short Presentation To Explain The Character of Uncle Sam, Made by Ivo BogoevskiIvo BogoevskiNessuna valutazione finora
- Brain Injury Patients Have A Place To Be Themselves: WHY WHYDocumento24 pagineBrain Injury Patients Have A Place To Be Themselves: WHY WHYDonna S. SeayNessuna valutazione finora
- Guidelines For Doing Business in Grenada & OECSDocumento14 pagineGuidelines For Doing Business in Grenada & OECSCharcoals Caribbean GrillNessuna valutazione finora
- Ty Baf TaxationDocumento4 pagineTy Baf TaxationAkki GalaNessuna valutazione finora
- Tax Havens IMF PDFDocumento59 pagineTax Havens IMF PDFClassic PhyXNessuna valutazione finora
- 2015 Student Handbook 16 January 2015Documento66 pagine2015 Student Handbook 16 January 2015John KhanNessuna valutazione finora
- New Presentation-Group AuditingDocumento23 pagineNew Presentation-Group Auditingrajes wariNessuna valutazione finora
- Chapter1 Intro To Basic FinanceDocumento28 pagineChapter1 Intro To Basic FinanceRazel GopezNessuna valutazione finora
- Data Science ProjectsDocumento3 pagineData Science ProjectsHanane GríssetteNessuna valutazione finora
- Financial Institutions Markets and ServicesDocumento2 pagineFinancial Institutions Markets and ServicesPavneet Kaur Bhatia100% (1)
- Learning Competency PDFDocumento1 paginaLearning Competency PDFLEOMAR PEUGALNessuna valutazione finora
- Revenue Memorandum Circular No. 55-2016: For ExampleDocumento2 pagineRevenue Memorandum Circular No. 55-2016: For ExampleFedsNessuna valutazione finora
- Unit 1 Bearer PlantsDocumento2 pagineUnit 1 Bearer PlantsEmzNessuna valutazione finora
- City Limits Magazine, December 1981 IssueDocumento28 pagineCity Limits Magazine, December 1981 IssueCity Limits (New York)Nessuna valutazione finora
- MSCM Dormitory Housing WEB UpdateDocumento12 pagineMSCM Dormitory Housing WEB Updatemax05XIIINessuna valutazione finora
- Sharat Babu Digumarti Vs State, Govt. of NCT of Delhi (Bazee - Com Case, Appeal) - Information Technology ActDocumento17 pagineSharat Babu Digumarti Vs State, Govt. of NCT of Delhi (Bazee - Com Case, Appeal) - Information Technology ActRavish Rana100% (1)
- EC 2012 With SolutionsDocumento50 pagineEC 2012 With Solutionsprabhjot singh1Nessuna valutazione finora
- ACC030 Comprehensive Project April2018 (Q)Documento5 pagineACC030 Comprehensive Project April2018 (Q)Fatin AkmalNessuna valutazione finora