Potrebbero piacerti anche
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (895)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- Drug StudyDocumento14 pagineDrug StudyWendy EscalanteNessuna valutazione finora
- Caring For The Bedridden PatientDocumento1 paginaCaring For The Bedridden PatientWendy EscalanteNessuna valutazione finora
- Assessment of Kidneys PDFDocumento1 paginaAssessment of Kidneys PDFWendy EscalanteNessuna valutazione finora
- NCPDocumento3 pagineNCPWendy EscalanteNessuna valutazione finora
- NCP 2 MiDocumento16 pagineNCP 2 MiWendy EscalanteNessuna valutazione finora
- PATHODocumento2 paginePATHOWendy EscalanteNessuna valutazione finora
- Nasogastric Tube Management and CareDocumento21 pagineNasogastric Tube Management and CareWendy EscalanteNessuna valutazione finora
- 02 Orig Art 02 PDFDocumento3 pagine02 Orig Art 02 PDFWendy EscalanteNessuna valutazione finora
- Modifiable Risk Factors Non - Modifiable Risk Factors: LegendDocumento2 pagineModifiable Risk Factors Non - Modifiable Risk Factors: LegendWendy Escalante100% (1)
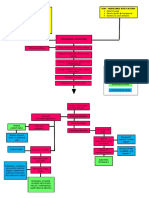
- Concept Map of Carotid Artery DiseaseDocumento2 pagineConcept Map of Carotid Artery DiseaseWendy EscalanteNessuna valutazione finora
- Acid-Ash DietDocumento10 pagineAcid-Ash DietWendy Escalante0% (1)
- Drug Study FinalDocumento8 pagineDrug Study FinalWendy EscalanteNessuna valutazione finora
- At DietDocumento8 pagineAt DietWendy EscalanteNessuna valutazione finora
- Brat DietDocumento8 pagineBrat DietWendy EscalanteNessuna valutazione finora
- Pediatric NursingDocumento16 paginePediatric NursingWendy Escalante100% (1)
- Assessment of KidneysDocumento1 paginaAssessment of KidneysWendy EscalanteNessuna valutazione finora
- Concept Map of CKD Gastrointestinal SymptomsDocumento4 pagineConcept Map of CKD Gastrointestinal SymptomsWendy Escalante0% (1)
- Degenerative Joint DiseaseDocumento35 pagineDegenerative Joint DiseaseWendy EscalanteNessuna valutazione finora
- Fundamentals in NursingDocumento9 pagineFundamentals in NursingWendy EscalanteNessuna valutazione finora
- Therapeutic DietDocumento3 pagineTherapeutic DietWendy EscalanteNessuna valutazione finora
- Case Presentation: Group 2Documento30 pagineCase Presentation: Group 2Wendy EscalanteNessuna valutazione finora
- DM Report1Documento16 pagineDM Report1Wendy EscalanteNessuna valutazione finora
- Nursing Care For Patient With Neurological DiseaseDocumento8 pagineNursing Care For Patient With Neurological DiseaseWendy EscalanteNessuna valutazione finora
- Integrated Management of Childhood Illness: Sick Child Age 2 Months Up To 5 YearsDocumento78 pagineIntegrated Management of Childhood Illness: Sick Child Age 2 Months Up To 5 YearsWendy EscalanteNessuna valutazione finora
- Diabetes MellitusDocumento5 pagineDiabetes MellitusWendy EscalanteNessuna valutazione finora
- FNCP CommunityDocumento4 pagineFNCP CommunityWendy EscalanteNessuna valutazione finora
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (400)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (588)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (74)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (345)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2259)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (121)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- FitnessDocumento3 pagineFitnessapi-301417711Nessuna valutazione finora
- AFA ReviwerDocumento21 pagineAFA ReviwerLovely day ybanezNessuna valutazione finora
- Tog 12228Documento7 pagineTog 12228Avanie PalNessuna valutazione finora
- 21 Benign Skin TumorsDocumento4 pagine21 Benign Skin TumorsAbdul Ghaffar AbdullahNessuna valutazione finora
- Community Health Nursing POST TEST Day 1Documento1 paginaCommunity Health Nursing POST TEST Day 1Mcbry TiongNessuna valutazione finora
- Pet Food 2Documento73 paginePet Food 2AB100% (1)
- Mechanisms of Ageing and Development: SciencedirectDocumento8 pagineMechanisms of Ageing and Development: SciencedirectAgustin LopezNessuna valutazione finora
- Recent Advances in The Management of Hypoxic-Ischemic Encephalopathy-IJPPDocumento6 pagineRecent Advances in The Management of Hypoxic-Ischemic Encephalopathy-IJPPdrtgodeNessuna valutazione finora
- MCN ReviewerDocumento5 pagineMCN ReviewerJunghoon YangParkNessuna valutazione finora
- Strategies For Feeding The Preterm Infant: ReviewDocumento10 pagineStrategies For Feeding The Preterm Infant: ReviewSanjuy GzzNessuna valutazione finora
- HypothesisDocumento4 pagineHypothesisSunny Boy Ng SinadjanNessuna valutazione finora
- Effect of Pre-Cooling Injection Site On Pain Perception in Pediatric Dentistry: "A Randomized Clinical Trial"Documento6 pagineEffect of Pre-Cooling Injection Site On Pain Perception in Pediatric Dentistry: "A Randomized Clinical Trial"Ummi AzizahNessuna valutazione finora
- Healing PowersDocumento9 pagineHealing PowersJack Key Chan AntigNessuna valutazione finora
- Lecture 5 - Facial Pain and TMJ DiseaseDocumento6 pagineLecture 5 - Facial Pain and TMJ DiseaseJeff ChadwickNessuna valutazione finora
- CL Septembre Grandma RemediesDocumento8 pagineCL Septembre Grandma RemediesMaria BenessalahNessuna valutazione finora
- Family Medicine PracticeDocumento510 pagineFamily Medicine PracticeIvan Ho100% (15)
- Symptoms and Signs: Compartment SyndromeDocumento4 pagineSymptoms and Signs: Compartment SyndromeajeikoNessuna valutazione finora
- IP Group 10 Making Soap Out of Guava LeavesDocumento5 pagineIP Group 10 Making Soap Out of Guava LeavesYuriko CaballeroNessuna valutazione finora
- TRS601 Vocabulary ListDocumento5 pagineTRS601 Vocabulary ListNgo Van Hung (K17 HCM)Nessuna valutazione finora
- Ncbi Selulitis BulosaDocumento3 pagineNcbi Selulitis BulosaHarefa TirtaNessuna valutazione finora
- Class 8 - Hand Shao-Yang San-Jiao ChannelDocumento89 pagineClass 8 - Hand Shao-Yang San-Jiao ChannelFrancisco VilaróNessuna valutazione finora
- 299.08 - Renal Pathology) Chronic Kideny Disease (CKD)Documento15 pagine299.08 - Renal Pathology) Chronic Kideny Disease (CKD)AnishilNessuna valutazione finora
- Plasmodium Infection (Malaria) : Medical ParasitologyDocumento7 paginePlasmodium Infection (Malaria) : Medical ParasitologyBalisi Manuel FranciscoNessuna valutazione finora
- Bakar CD RobiwijayaDocumento60 pagineBakar CD RobiwijayaAsep Ribbat MNessuna valutazione finora
- Jpog August 2013 IdDocumento51 pagineJpog August 2013 IdHasyim PurwadiNessuna valutazione finora
- Digestive System Charts 1Documento14 pagineDigestive System Charts 1api-306762527Nessuna valutazione finora
- 1187 FullDocumento7 pagine1187 FullPrincessDianna SulitNessuna valutazione finora
- Management of Cancer (Dr. Lim)Documento6 pagineManagement of Cancer (Dr. Lim)Miguel Cuevas DolotNessuna valutazione finora
- 2 Upper Airway Disorders PDFDocumento33 pagine2 Upper Airway Disorders PDFMonica BorjaNessuna valutazione finora
- Classification of Psychiatric DisordersDocumento64 pagineClassification of Psychiatric Disordersdrkadiyala2100% (1)