Potrebbero piacerti anche
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (895)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (344)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (121)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (74)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- Process Safety - Recommended Practice On KPIsDocumento36 pagineProcess Safety - Recommended Practice On KPIsKB100% (2)
- (2012) (IEEE) Multi-Tank Fuzzy Level Controller System Using KinectDocumento5 pagine(2012) (IEEE) Multi-Tank Fuzzy Level Controller System Using KinectOscar AvilesNessuna valutazione finora
- (2016) (IJAER) Active Suspension Control Proposal For A Six-Wheeled Autonomous CarDocumento10 pagine(2016) (IJAER) Active Suspension Control Proposal For A Six-Wheeled Autonomous CarOscar AvilesNessuna valutazione finora
- (2018) (Medwell) SP Design of A Mechatronic Device For Measuring Stump Stresses On Transfemoral AmputeesDocumento7 pagine(2018) (Medwell) SP Design of A Mechatronic Device For Measuring Stump Stresses On Transfemoral AmputeesOscar AvilesNessuna valutazione finora
- (2020) (IJASEIT) SP Modeling and Simulation of A DC Micro Grid With A Model PredictiveDocumento8 pagine(2020) (IJASEIT) SP Modeling and Simulation of A DC Micro Grid With A Model PredictiveOscar AvilesNessuna valutazione finora
- (2016) (IJAER) Comparison of Control Methods For Modular Robotic SystemsDocumento14 pagine(2016) (IJAER) Comparison of Control Methods For Modular Robotic SystemsOscar AvilesNessuna valutazione finora
- Hybrid Brain-Computer Interface Techniques For Improved Classification Accuracy and Increased Number of Commands: A ReviewDocumento27 pagineHybrid Brain-Computer Interface Techniques For Improved Classification Accuracy and Increased Number of Commands: A ReviewOscar AvilesNessuna valutazione finora
- (2016) (INDJST) Analysis of Autoregressive Predictive Models and Artificial Neural Networks For Irradiance EstimationDocumento20 pagine(2016) (INDJST) Analysis of Autoregressive Predictive Models and Artificial Neural Networks For Irradiance EstimationOscar AvilesNessuna valutazione finora
- (2016) (Ijoee) Fuzzy Control For Solar Photovoltaic Tracking SystemDocumento4 pagine(2016) (Ijoee) Fuzzy Control For Solar Photovoltaic Tracking SystemOscar AvilesNessuna valutazione finora
- (2020) (TRPJ) Sliding Mode Control of A Planar MechanismDocumento16 pagine(2020) (TRPJ) Sliding Mode Control of A Planar MechanismOscar AvilesNessuna valutazione finora
- (2019) (Ijmet) Upper Extremity Exoskeleton For Teleoperation of Hybrid RobotDocumento15 pagine(2019) (Ijmet) Upper Extremity Exoskeleton For Teleoperation of Hybrid RobotOscar AvilesNessuna valutazione finora
- (2019) (MUSME) Exoskeleton Glove With Cable Driven Fingers Actuated by A Differential MechanismDocumento23 pagine(2019) (MUSME) Exoskeleton Glove With Cable Driven Fingers Actuated by A Differential MechanismOscar AvilesNessuna valutazione finora
- (2020) (JAST) Analysis of The Behavior of The Artificial PancreasDocumento21 pagine(2020) (JAST) Analysis of The Behavior of The Artificial PancreasOscar AvilesNessuna valutazione finora
- 8 (2020) (JAST) Analysis and Simulation of The Couple Direct Kinematics of A 6 Wheeled Mobile Platform With A 3 DOF Manipulator ArmDocumento16 pagine8 (2020) (JAST) Analysis and Simulation of The Couple Direct Kinematics of A 6 Wheeled Mobile Platform With A 3 DOF Manipulator ArmOscar AvilesNessuna valutazione finora
- (2020) (TRPJ) Experimental Approach To The Design of The Links of A Delta RobotDocumento19 pagine(2020) (TRPJ) Experimental Approach To The Design of The Links of A Delta RobotOscar AvilesNessuna valutazione finora
- Presentación JANITO VAQUEIRO PDFDocumento81 paginePresentación JANITO VAQUEIRO PDFOscar AvilesNessuna valutazione finora
- Notas de Sistemas DinamicosDocumento75 pagineNotas de Sistemas DinamicosOscar AvilesNessuna valutazione finora
- (2020) (JAST) Finger Prosthetic Design Based in The Anatomy and Biomechanics StudiesDocumento18 pagine(2020) (JAST) Finger Prosthetic Design Based in The Anatomy and Biomechanics StudiesOscar AvilesNessuna valutazione finora
- 4 (2020) (JAST) Discrete Generalized PI Control Applied To A DC-DC Converter With A Coupled MotorDocumento18 pagine4 (2020) (JAST) Discrete Generalized PI Control Applied To A DC-DC Converter With A Coupled MotorOscar AvilesNessuna valutazione finora
- (2020) (UPC-JAST) Application of Neural Networks For Image Analysis of MagneticDocumento12 pagine(2020) (UPC-JAST) Application of Neural Networks For Image Analysis of MagneticOscar AvilesNessuna valutazione finora
- (2020) (IJAST) Exoskeletons For Rehabilitation in Motor ImpairmentsDocumento13 pagine(2020) (IJAST) Exoskeletons For Rehabilitation in Motor ImpairmentsOscar AvilesNessuna valutazione finora
- Automatic Dog FeederDocumento14 pagineAutomatic Dog FeederOscar AvilesNessuna valutazione finora
- Formulario de Sistemas de ControlDocumento10 pagineFormulario de Sistemas de ControlRuben VelazquezNessuna valutazione finora
- ECE 486: A Note On SensitivityDocumento2 pagineECE 486: A Note On SensitivityOscar AvilesNessuna valutazione finora
- Hardarwe in The LoopDocumento6 pagineHardarwe in The LoopOscar AvilesNessuna valutazione finora
- Modelling of Manipulators RobotsDocumento133 pagineModelling of Manipulators RobotsOscar AvilesNessuna valutazione finora
- Introduction To Control SystemsDocumento3 pagineIntroduction To Control SystemsOscar AvilesNessuna valutazione finora
- Mathetical ModelDocumento3 pagineMathetical ModelOscar AvilesNessuna valutazione finora
- (2015) Identificacon de Patologias Basado en Presión PlantarDocumento17 pagine(2015) Identificacon de Patologias Basado en Presión PlantarOscar AvilesNessuna valutazione finora
- Intro To MechatronicsDocumento33 pagineIntro To MechatronicscorozcogarciaNessuna valutazione finora
- Certifier FA English 1980436 PDFDocumento42 pagineCertifier FA English 1980436 PDFRafa TejedaNessuna valutazione finora
- Advanced Construction MaterialsDocumento37 pagineAdvanced Construction MaterialsZara AliNessuna valutazione finora
- Fire Pump AccessoriesDocumento23 pagineFire Pump AccessoriesMuhammad ArslanNessuna valutazione finora
- SOP For Sampling and Testing Schedule of Water For Injection and Clean Steam - Pharmaceutical GuidelinesDocumento2 pagineSOP For Sampling and Testing Schedule of Water For Injection and Clean Steam - Pharmaceutical GuidelinesASHOK KUMAR LENKA100% (1)
- Landing NippleDocumento4 pagineLanding NippleMohamed Abd El-MoniemNessuna valutazione finora
- Preparation of Tin TetraiodideDocumento2 paginePreparation of Tin Tetraiodidestudent_4_evaNessuna valutazione finora
- 17.salt Aluminium Sulphate 3Documento3 pagine17.salt Aluminium Sulphate 3Sarthika GaulkarNessuna valutazione finora
- PD 984Documento38 paginePD 984mav3riick100% (2)
- Documents - Tips Direct Determination of Tin in Whole Blood and Urine by GF AasDocumento5 pagineDocuments - Tips Direct Determination of Tin in Whole Blood and Urine by GF AasRozzy RamanandaNessuna valutazione finora
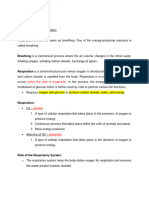
- Biology Notes - Respiratory SystemDocumento9 pagineBiology Notes - Respiratory SystemnoorbdeirNessuna valutazione finora
- Nato - Stanag 4582 - Explosives, Nitrocellulose Based Propellants, Stability Test Procedure and Requirements Using Heat Flow CalorimetryDocumento25 pagineNato - Stanag 4582 - Explosives, Nitrocellulose Based Propellants, Stability Test Procedure and Requirements Using Heat Flow CalorimetryTetis BrionesNessuna valutazione finora
- Appendix C - ART Windcube Lidar v2.1 Maintenance - v02Documento2 pagineAppendix C - ART Windcube Lidar v2.1 Maintenance - v02Vo Quang Kiet (ヴォー クァン キエット)Nessuna valutazione finora
- In-Vitro Antimicrobial Activity of Nano-Chitosan Hydroxyapatite Against Streptococcus Mutans On Biofilm FormationDocumento8 pagineIn-Vitro Antimicrobial Activity of Nano-Chitosan Hydroxyapatite Against Streptococcus Mutans On Biofilm FormationInternational Journal of Innovative Science and Research TechnologyNessuna valutazione finora
- 13CrMo45 P12 T12 Engl PDFDocumento3 pagine13CrMo45 P12 T12 Engl PDFYankMulya MusaNessuna valutazione finora
- WAEC Chemistry Syllabus 2022 PDF Download AvailableDocumento26 pagineWAEC Chemistry Syllabus 2022 PDF Download AvailableSamuel AikinsNessuna valutazione finora
- Phoenicia University Department of Engineering Faculty of Petroleum Engineering Petroleum Fluid Properties Laboratory PENG212L Dean Stark Plug SizeDocumento14 paginePhoenicia University Department of Engineering Faculty of Petroleum Engineering Petroleum Fluid Properties Laboratory PENG212L Dean Stark Plug SizeEmanuelta NaibahoNessuna valutazione finora
- Basics of SMAWDocumento157 pagineBasics of SMAWAsad Bin Ala QatariNessuna valutazione finora
- Understanding Vacuum Pump LubricantsDocumento21 pagineUnderstanding Vacuum Pump LubricantsengrsurifNessuna valutazione finora
- Odorcarb Ultra Media SDS (GHS v1.01)Documento8 pagineOdorcarb Ultra Media SDS (GHS v1.01)jeanjean283Nessuna valutazione finora
- Scat PornDocumento72 pagineScat PornCallum Biggs0% (1)
- Terwet 105 MSDSDocumento6 pagineTerwet 105 MSDSLuki WahyudiNessuna valutazione finora
- 19 Pulv - MSDSDocumento11 pagine19 Pulv - MSDSLam NgọcNessuna valutazione finora
- Grasim Compre ReportDocumento60 pagineGrasim Compre ReportManas KalraNessuna valutazione finora
- Chapter 3-Structure and Stereochemistry of Alkanes: N 2n+2 27 56 N 2n+2 42 86Documento18 pagineChapter 3-Structure and Stereochemistry of Alkanes: N 2n+2 27 56 N 2n+2 42 86張湧浩Nessuna valutazione finora
- LSH 8 Steps To Mapping Validation ProjectDocumento20 pagineLSH 8 Steps To Mapping Validation ProjecthuykhiemNessuna valutazione finora
- Artículo para ForoDocumento7 pagineArtículo para ForoJuan MendozaNessuna valutazione finora
- Plumbing Piping For Building: NIOEC-SP-30-05Documento9 paginePlumbing Piping For Building: NIOEC-SP-30-05masoud132Nessuna valutazione finora
- MSDS - Prominent-GlycineDocumento6 pagineMSDS - Prominent-GlycineTanawat ChinchaivanichkitNessuna valutazione finora