Potrebbero piacerti anche
- Sample Case Presentation - Occult BacteremiaDocumento51 pagineSample Case Presentation - Occult BacteremiaPrecious Gutierrez BagazinNessuna valutazione finora
- Lapjag Bangsal IPD 22 OKTOBER DHFDocumento57 pagineLapjag Bangsal IPD 22 OKTOBER DHFLeony Nerry SabatiniNessuna valutazione finora
- Apriyanto Lifandy Desmy FadillahDocumento38 pagineApriyanto Lifandy Desmy FadillahdesmyyNessuna valutazione finora
- CKDDocumento48 pagineCKDJuniorNessuna valutazione finora
- Polymyalgia RheumaticaDocumento23 paginePolymyalgia RheumaticaGabriella TungadiNessuna valutazione finora
- Morning Endorsement: Group 10 - Subgroup 1Documento30 pagineMorning Endorsement: Group 10 - Subgroup 1Kevin MarquezNessuna valutazione finora
- Pleurak EffusionDocumento16 paginePleurak EffusionElfriska SihombingNessuna valutazione finora
- Duty Report Highlights Doctor and Patient DetailsDocumento25 pagineDuty Report Highlights Doctor and Patient DetailsAuditya WidyasariNessuna valutazione finora
- These Are Hospital PresentationsDocumento73 pagineThese Are Hospital PresentationsMahmoud AjinehNessuna valutazione finora
- TYPHOID FEVER Morport InternaDocumento17 pagineTYPHOID FEVER Morport InternapoonpatchaNessuna valutazione finora
- Community Acquired PneumoniaDocumento56 pagineCommunity Acquired Pneumoniashiean06Nessuna valutazione finora
- Approach To Cough: Mark Angelo Z. Ponferrado, MD Pre-ResidentDocumento32 pagineApproach To Cough: Mark Angelo Z. Ponferrado, MD Pre-ResidentMark Angelo PonferradoNessuna valutazione finora
- Rheumatology Division Case ReportDocumento25 pagineRheumatology Division Case ReporttomeyttoNessuna valutazione finora
- Acute Nephrotic SyndromeDocumento10 pagineAcute Nephrotic SyndromeEvi SilviaNessuna valutazione finora
- Morning Endorsement: Group 9 Subgroup 2Documento36 pagineMorning Endorsement: Group 9 Subgroup 2Kevin MarquezNessuna valutazione finora
- Postpartum Hemorrhage Case PresentationDocumento44 paginePostpartum Hemorrhage Case PresentationRose Anne Kunz Simbulan100% (1)
- Community-Acquired Pneumonia GuideDocumento37 pagineCommunity-Acquired Pneumonia GuideKristine-Joy Legaspi FrancoNessuna valutazione finora
- MR Abdul Muthalib OADocumento20 pagineMR Abdul Muthalib OAfadli padoNessuna valutazione finora
- AdconDocumento25 pagineAdconAnna AlcantaraNessuna valutazione finora
- Case Presentation: BY 13QO320Documento15 pagineCase Presentation: BY 13QO320Sandeep ChakravarthyNessuna valutazione finora
- DengueDocumento38 pagineDengueadetiquezNessuna valutazione finora
- Typhoid FeverDocumento68 pagineTyphoid FeverLd Rachel PableoNessuna valutazione finora
- Morning Endorsement: October 7, 2020 Group 10 - Subgroup 3Documento26 pagineMorning Endorsement: October 7, 2020 Group 10 - Subgroup 3Deomicah SolanoNessuna valutazione finora
- LAPKAS-Elsa Nur Rahma Diahnissa-2016730030-1Documento34 pagineLAPKAS-Elsa Nur Rahma Diahnissa-2016730030-1Raka WibisonoNessuna valutazione finora
- Lupus Case PresentationDocumento48 pagineLupus Case PresentationRoscelie KhoNessuna valutazione finora
- Final CaseDocumento45 pagineFinal Case_carido_Nessuna valutazione finora
- MORNING REPORT CASEDocumento22 pagineMORNING REPORT CASESunardiasihNessuna valutazione finora
- Pedia BAIEDocumento49 paginePedia BAIEDarlene Clarice V. LabacladoNessuna valutazione finora
- Adult Onset Henöch-Schonlein Purpura - A Case ReportDocumento22 pagineAdult Onset Henöch-Schonlein Purpura - A Case ReportDan MariciucNessuna valutazione finora
- Case Report Systemic Lupus Erythematosus: WIDYA AULIA C014182261 Siti Azreen Azira Binti Adzhar C014182197Documento35 pagineCase Report Systemic Lupus Erythematosus: WIDYA AULIA C014182261 Siti Azreen Azira Binti Adzhar C014182197ghaisani humairahNessuna valutazione finora
- Typhoid Case PresentationDocumento79 pagineTyphoid Case PresentationJulius Dominique L. AnjaoNessuna valutazione finora
- Neli Pastinar, Penkes UE, RPGN, SLE, Duty HannaDocumento19 pagineNeli Pastinar, Penkes UE, RPGN, SLE, Duty HannaHanna GustinNessuna valutazione finora
- Case Report Ward Wednesday, 11/01/2017: Ward GP: Dr. Widya An'umillah FarellaDocumento39 pagineCase Report Ward Wednesday, 11/01/2017: Ward GP: Dr. Widya An'umillah FarellaFarella KartikaNessuna valutazione finora
- Acute Rheumatic FeverDocumento37 pagineAcute Rheumatic FeverQadriyah Ramadhani100% (1)
- Grand ReportsDocumento60 pagineGrand ReportsfilchibuffNessuna valutazione finora
- Breathlessness Lung CancerDocumento13 pagineBreathlessness Lung CancerElsy Pramitha SariNessuna valutazione finora
- AnemiaDocumento62 pagineAnemiaKay Ramos JimenoNessuna valutazione finora
- Gout Arthritis Acute: Case ReportDocumento44 pagineGout Arthritis Acute: Case ReportAgung Sukriadi HarliNessuna valutazione finora
- Case Presentation BronchiectasisDocumento61 pagineCase Presentation BronchiectasisUzair Muhd100% (6)
- Lapkas AppendisitisDocumento37 pagineLapkas AppendisitisM Izzudin IkhwanNessuna valutazione finora
- Edited CapDocumento81 pagineEdited CapSimon Peter MollanedaNessuna valutazione finora
- Case Presentation SanjidaDocumento41 pagineCase Presentation SanjidascarletsanjidaNessuna valutazione finora
- Stemi Anteroseptal: Onset 6 Hours Killip IiDocumento35 pagineStemi Anteroseptal: Onset 6 Hours Killip IiirmaarmiyahNessuna valutazione finora
- Case Presentation: Cagayan Valley Medical CenterDocumento57 pagineCase Presentation: Cagayan Valley Medical CenterGian PagadduNessuna valutazione finora
- Dengue CaseDocumento23 pagineDengue CaseMary SheshiraNessuna valutazione finora
- Baby Boy 6 Month Old: Genera L DataDocumento47 pagineBaby Boy 6 Month Old: Genera L DataJanseen EdizaNessuna valutazione finora
- Syafrudin, Male, 58 Yo, MW 11: Chief Complaint: (Autoanamnesis and Alloanamnesis) Present Illness HistoryDocumento14 pagineSyafrudin, Male, 58 Yo, MW 11: Chief Complaint: (Autoanamnesis and Alloanamnesis) Present Illness HistoryLukman NurhakimNessuna valutazione finora
- Morep Interna 2 Oktober 2015Documento18 pagineMorep Interna 2 Oktober 2015dyansaNessuna valutazione finora
- Case Report: Hepatitis BDocumento34 pagineCase Report: Hepatitis Bdewi sartikaNessuna valutazione finora
- Duty Report On Ward 24-06-15Documento25 pagineDuty Report On Ward 24-06-15Annisa Rizki Ratih PratiwiNessuna valutazione finora
- MR Interna Intoksikasi MetanolDocumento17 pagineMR Interna Intoksikasi Metanolvina_vermillionNessuna valutazione finora
- Case-Presentation 2Documento28 pagineCase-Presentation 2Ugalde AlyssakyleNessuna valutazione finora
- A Case Presentation - PediaDocumento50 pagineA Case Presentation - PediaCathy ChiongNessuna valutazione finora
- Medicine Admitting Conference: University of Santo Tomas Faculty of Medicine and SurgeryDocumento70 pagineMedicine Admitting Conference: University of Santo Tomas Faculty of Medicine and SurgerySTEPHANIE TANNessuna valutazione finora
- Morning Report Gastroenteritis CaseDocumento12 pagineMorning Report Gastroenteritis CasezakyalfathuNessuna valutazione finora
- Morning Report - 12 Juli 2016Documento21 pagineMorning Report - 12 Juli 2016Hanna G. FauziaNessuna valutazione finora
- Acute Lymphoblastic LeukemiaDocumento20 pagineAcute Lymphoblastic LeukemiazahraaNessuna valutazione finora
- SLE - Kulah FKUMJ 2010 FkkumjDocumento56 pagineSLE - Kulah FKUMJ 2010 Fkkumjzam zamiNessuna valutazione finora
- A Child With Prolonged FeverDocumento38 pagineA Child With Prolonged FeverAly MorsyNessuna valutazione finora
- Dengue Deepak 2016 Version OneDocumento57 pagineDengue Deepak 2016 Version OneDeepak GhimireNessuna valutazione finora
- Arteries and Vein of Head and Neck PDFDocumento24 pagineArteries and Vein of Head and Neck PDFDeepak GhimireNessuna valutazione finora
- Types of ReflexDocumento1 paginaTypes of ReflexDeepak GhimireNessuna valutazione finora
- Smoking CessationDocumento1 paginaSmoking CessationDeepak GhimireNessuna valutazione finora
- Diagnosis, Treatment, and Prevention of Typhoid Fever (WHO)Documento48 pagineDiagnosis, Treatment, and Prevention of Typhoid Fever (WHO)Nina KharimaNessuna valutazione finora
- ToxicityDocumento2 pagineToxicityDeepak GhimireNessuna valutazione finora
- Ruptured ectopic pregnancyDocumento59 pagineRuptured ectopic pregnancyDeepak GhimireNessuna valutazione finora
- Arteries and Vein of Head and NeckDocumento24 pagineArteries and Vein of Head and NeckDeepak GhimireNessuna valutazione finora
- Gout CPG Manuscript - PJIM 072808Documento16 pagineGout CPG Manuscript - PJIM 072808Francis CastellNessuna valutazione finora
- Echocardiography DeepakDocumento71 pagineEchocardiography DeepakDeepak Ghimire88% (8)
- Viral Exanthems: Study Online atDocumento2 pagineViral Exanthems: Study Online atDeepak GhimireNessuna valutazione finora
- DTDocumento1 paginaDTDeepak GhimireNessuna valutazione finora
- Hernia Treatment GeneralDocumento2 pagineHernia Treatment GeneralDeepak GhimireNessuna valutazione finora
- ToxicityDocumento2 pagineToxicityDeepak GhimireNessuna valutazione finora
- Wisdom Eye of BuddhaDocumento1 paginaWisdom Eye of BuddhaDeepak GhimireNessuna valutazione finora
- Buddha's Wisdom EyeDocumento1 paginaBuddha's Wisdom EyeDeepak GhimireNessuna valutazione finora
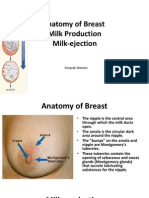
- Anatomy of Breast, Milk Production, and Milk-EjectionDocumento23 pagineAnatomy of Breast, Milk Production, and Milk-EjectionDeepak Ghimire100% (2)
- Villaluz: Hypertensive Disorders, Multifetal Pregnancy, Preterm BirthDocumento1 paginaVillaluz: Hypertensive Disorders, Multifetal Pregnancy, Preterm BirthDeepak GhimireNessuna valutazione finora
- Introduction To Cosmetic SurgeryDocumento2 pagineIntroduction To Cosmetic SurgeryDeepak GhimireNessuna valutazione finora
- Endocrine SystemDocumento41 pagineEndocrine SystemDeepak Ghimire0% (1)
- Sexual Response LectureDocumento18 pagineSexual Response LectureDeepak GhimireNessuna valutazione finora
- Endocrine SystemDocumento41 pagineEndocrine SystemDeepak Ghimire0% (1)
- Student Council 2014/15: ExclusiveDocumento3 pagineStudent Council 2014/15: ExclusiveDeepak GhimireNessuna valutazione finora
- ReconstructionDocumento75 pagineReconstructionDeepak GhimireNessuna valutazione finora
- Sleeping Disorders (Somnipathy)Documento13 pagineSleeping Disorders (Somnipathy)Deepak GhimireNessuna valutazione finora
- ParasitologiiDocumento40 pagineParasitologiiRabecca TobingNessuna valutazione finora
- Passport Application FormDocumento1 paginaPassport Application FormAl HasaNessuna valutazione finora
- Clinical Anatomy of Abdominal RegionDocumento11 pagineClinical Anatomy of Abdominal RegionDeepak GhimireNessuna valutazione finora
- Approach Neurologic DiagnosisDocumento8 pagineApproach Neurologic DiagnosisDeepak GhimireNessuna valutazione finora
- Dimension Exl 200 Tech SpecsDocumento2 pagineDimension Exl 200 Tech SpecsOo Kenx OoNessuna valutazione finora
- Test-11 (Current Affair-2)Documento86 pagineTest-11 (Current Affair-2)Pavansaikumar DasariNessuna valutazione finora
- CNH Construction Health DeclarationDocumento1 paginaCNH Construction Health DeclarationEna Ahmad PieNessuna valutazione finora
- Unseen PassageDocumento7 pagineUnseen PassageVinay OjhaNessuna valutazione finora
- Science Learning Sheet 1 RESPIRATORY SYSTEMDocumento3 pagineScience Learning Sheet 1 RESPIRATORY SYSTEMexelainedivineNessuna valutazione finora
- Guidelines For Distt Hospitals - Indian Public Health StandardsDocumento124 pagineGuidelines For Distt Hospitals - Indian Public Health StandardsTejinder SinghNessuna valutazione finora
- Ranula: A Review of LiteratureDocumento6 pagineRanula: A Review of LiteratureNicco MarantsonNessuna valutazione finora
- Diabetes Mellitus: DefinitionDocumento95 pagineDiabetes Mellitus: DefinitionMalik Rizwan ElahiNessuna valutazione finora
- Case Scenario: Self-Risk AssessmentDocumento2 pagineCase Scenario: Self-Risk AssessmentAlyanna Alcazar CapateNessuna valutazione finora
- Elective Caesarean Section on a GoatDocumento17 pagineElective Caesarean Section on a GoatAbdirazak AlkhaalidNessuna valutazione finora
- Nettle Rash Symptoms, Causes, TreatmentDocumento2 pagineNettle Rash Symptoms, Causes, TreatmentArdave Laurente100% (1)
- Envis Newsletter April 2014Documento16 pagineEnvis Newsletter April 2014Mikel MillerNessuna valutazione finora
- Ameloblastoma: Notorious Tumor of The Jaw - Report of A CaseDocumento3 pagineAmeloblastoma: Notorious Tumor of The Jaw - Report of A CaseUwie MoumootNessuna valutazione finora
- Aapi Ebook June 19 2017Documento621 pagineAapi Ebook June 19 2017AAPIUSANessuna valutazione finora
- Transfusion-Related Acute Lung Injury: HistoryDocumento20 pagineTransfusion-Related Acute Lung Injury: HistoryBladimir CentenoNessuna valutazione finora
- 2019-04-01 Good Housekeeping PDFDocumento126 pagine2019-04-01 Good Housekeeping PDFTiểu MyNessuna valutazione finora
- Routine Use of Vitamin K in The Treatment of Cirrhosis-Related Coagulopathy: Is It A-O-K? Maybe Not, We SayDocumento6 pagineRoutine Use of Vitamin K in The Treatment of Cirrhosis-Related Coagulopathy: Is It A-O-K? Maybe Not, We Sayannisa edwarNessuna valutazione finora
- MUSYAWARAH GURU MATA PELAJARAN BAHASA INGGRIS UJIAN SEKOLAHDocumento13 pagineMUSYAWARAH GURU MATA PELAJARAN BAHASA INGGRIS UJIAN SEKOLAHASEP MALIKNessuna valutazione finora
- AcupunctureDocumento15 pagineAcupuncturezextorcNessuna valutazione finora
- DR.ZHU'S SCALP ACUPUNCTURE GUIDEDocumento25 pagineDR.ZHU'S SCALP ACUPUNCTURE GUIDEMajid Mushtaq100% (2)
- MidtermDocumento22 pagineMidtermEmvie Loyd Pagunsan-ItableNessuna valutazione finora
- Effectiveness of 6 Step Prevention and Control For Dengue Hemorrhagic Fever in Rural Community of ThailandDocumento142 pagineEffectiveness of 6 Step Prevention and Control For Dengue Hemorrhagic Fever in Rural Community of ThailandMendoza Alech ChelaNessuna valutazione finora
- GRANDE ICU CASE SUMMARYDocumento3 pagineGRANDE ICU CASE SUMMARYanuzNessuna valutazione finora
- EHSMS Performance and Incident ReportingDocumento38 pagineEHSMS Performance and Incident ReportingravimanasNessuna valutazione finora
- Yellow Fever Vaccination Requirements From India - Chalo AfricaDocumento148 pagineYellow Fever Vaccination Requirements From India - Chalo AfricaAbishek ChandranNessuna valutazione finora
- Managing Cardiac Patients in the ICUDocumento26 pagineManaging Cardiac Patients in the ICUvamshidh100% (2)
- Rapyuta Robotics PVT LTD - GMC Renewal Quote - 28th Dec2022Documento1 paginaRapyuta Robotics PVT LTD - GMC Renewal Quote - 28th Dec2022nagarajgnairyNessuna valutazione finora
- Food For The BrainDocumento34 pagineFood For The BrainKristine Mae AbrasaldoNessuna valutazione finora
- Cattle InsuranceDocumento8 pagineCattle Insurancebharti ashhplayNessuna valutazione finora
- New Drugs 2014-2018Documento31 pagineNew Drugs 2014-2018Prem Goel0% (1)