Potrebbero piacerti anche
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (895)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (344)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (121)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (73)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- Weather Prediction Using Machine Learning TechniquessDocumento53 pagineWeather Prediction Using Machine Learning Techniquessbakiz89Nessuna valutazione finora
- Method Statement For Construction of Concrete Batching Plant (Combined)Documento72 pagineMethod Statement For Construction of Concrete Batching Plant (Combined)NP Dien100% (1)
- Anaemia of Chronic Kidney Diseas8 PDFDocumento49 pagineAnaemia of Chronic Kidney Diseas8 PDFDevi Resmi SariNessuna valutazione finora
- Puskesmas Rawat InapDocumento1 paginaPuskesmas Rawat InapbangunazhariyusufNessuna valutazione finora
- Biology of Tendon Injury: Healing, Modeling and Remodeling: P. Sharma and N. MaffulliDocumento10 pagineBiology of Tendon Injury: Healing, Modeling and Remodeling: P. Sharma and N. MaffulliBrianna RyanNessuna valutazione finora
- Food Challenge TestDocumento2 pagineFood Challenge TestbangunazhariyusufNessuna valutazione finora
- Complicated Periorbital Cellulitis Case ReportDocumento4 pagineComplicated Periorbital Cellulitis Case ReportbangunazhariyusufNessuna valutazione finora
- Anaemia of Chronic Kidney Diseas8 PDFDocumento49 pagineAnaemia of Chronic Kidney Diseas8 PDFDevi Resmi SariNessuna valutazione finora
- Extensor Tendon Injury ProtocolDocumento11 pagineExtensor Tendon Injury ProtocoltasneempichoriNessuna valutazione finora
- Management of Extensor Tendon InjuriesDocumento7 pagineManagement of Extensor Tendon InjurieskenthepaNessuna valutazione finora
- Achilles Tendon RuptureDocumento11 pagineAchilles Tendon RupturebangunazhariyusufNessuna valutazione finora
- Ruptur Tendon AchillesDocumento18 pagineRuptur Tendon AchillesAulya Novaldy PratomoNessuna valutazione finora
- Ruptured Foot Tendon: Background & Etiology (Cause)Documento4 pagineRuptured Foot Tendon: Background & Etiology (Cause)bangunazhariyusufNessuna valutazione finora
- Achilles Tendon RuptureDocumento6 pagineAchilles Tendon RupturechloramphenicolNessuna valutazione finora
- Spontaneous Bilateral Achilles Tendon RuptureDocumento5 pagineSpontaneous Bilateral Achilles Tendon RupturebangunazhariyusufNessuna valutazione finora
- Does Prolonged Length of Stay in The Emergency DepartmentDocumento9 pagineDoes Prolonged Length of Stay in The Emergency DepartmentbangunazhariyusufNessuna valutazione finora
- Lateralization in Cluster Headache A Nordic Multicenter StudyDocumento6 pagineLateralization in Cluster Headache A Nordic Multicenter StudybangunazhariyusufNessuna valutazione finora
- Achilles Tendon RuptureDocumento11 pagineAchilles Tendon RupturebangunazhariyusufNessuna valutazione finora
- Thyroid-Stimulating Hormone, White MatterDocumento8 pagineThyroid-Stimulating Hormone, White MatterbangunazhariyusufNessuna valutazione finora
- Brainstem Infarcts Predict REM Sleep BehaviorDocumento5 pagineBrainstem Infarcts Predict REM Sleep BehaviorbangunazhariyusufNessuna valutazione finora
- Facial Nerve Decompression For Idiopathic Bell's PalsyDocumento8 pagineFacial Nerve Decompression For Idiopathic Bell's PalsybangunazhariyusufNessuna valutazione finora
- The Effect of Early Neuromuscular ElectricalDocumento7 pagineThe Effect of Early Neuromuscular ElectricalhasNessuna valutazione finora
- Ameloblastoma in The MandibleDocumento1 paginaAmeloblastoma in The MandiblebangunazhariyusufNessuna valutazione finora
- Lateralization in Cluster Headache A Nordic Multicenter StudyDocumento6 pagineLateralization in Cluster Headache A Nordic Multicenter StudybangunazhariyusufNessuna valutazione finora
- Facial Nerve Decompression For Idiopathic Bell's PalsyDocumento8 pagineFacial Nerve Decompression For Idiopathic Bell's PalsybangunazhariyusufNessuna valutazione finora
- Classification and Clinical Features of Headache PatientsDocumento8 pagineClassification and Clinical Features of Headache PatientsbangunazhariyusufNessuna valutazione finora
- Cover Proposal BayuDocumento7 pagineCover Proposal BayubangunazhariyusufNessuna valutazione finora
- SkrofulodermaDocumento4 pagineSkrofulodermabangunazhariyusufNessuna valutazione finora
- Antibacterial and Antifungal Properties of Human CerumenDocumento1 paginaAntibacterial and Antifungal Properties of Human CerumenbangunazhariyusufNessuna valutazione finora
- Attitude of Tribal and Non Tribal Students Towards ModernizationDocumento9 pagineAttitude of Tribal and Non Tribal Students Towards ModernizationAnonymous CwJeBCAXpNessuna valutazione finora
- KKS Equipment Matrik No PM Description PM StartDocumento3 pagineKKS Equipment Matrik No PM Description PM StartGHAZY TUBeNessuna valutazione finora
- Nursing Care Plan For AIDS HIVDocumento3 pagineNursing Care Plan For AIDS HIVFARAH MAE MEDINA100% (2)
- Statistics and Probability Course Syllabus (2023) - SignedDocumento3 pagineStatistics and Probability Course Syllabus (2023) - SignedDarence Fujihoshi De AngelNessuna valutazione finora
- Open Book Online: Syllabus & Pattern Class - XiDocumento1 paginaOpen Book Online: Syllabus & Pattern Class - XiaadityaNessuna valutazione finora
- The 100 Best Books For 1 Year Olds: Board Book HardcoverDocumento17 pagineThe 100 Best Books For 1 Year Olds: Board Book Hardcovernellie_74023951Nessuna valutazione finora
- Hydrotest Test FormatDocumento27 pagineHydrotest Test FormatRähûl Prätäp SïnghNessuna valutazione finora
- Archetypal Approach To Macbeth by William ShakespeareDocumento9 pagineArchetypal Approach To Macbeth by William ShakespeareLenka Koutná100% (1)
- Contemporary Architecture Is The Architecture of The 21st Century. No Single Style Is DominantDocumento2 pagineContemporary Architecture Is The Architecture of The 21st Century. No Single Style Is DominantShubham DuaNessuna valutazione finora
- TextdocumentDocumento254 pagineTextdocumentSaurabh SihagNessuna valutazione finora
- Saunders & Cornnet Solution Chapter 1 Part 1Documento5 pagineSaunders & Cornnet Solution Chapter 1 Part 1Mo AlamNessuna valutazione finora
- DGKCC Internship ReportDocumento17 pagineDGKCC Internship ReportMuhammad AtharNessuna valutazione finora
- Operaciones UnitariasDocumento91 pagineOperaciones UnitariasAlejandro ReyesNessuna valutazione finora
- NRNP PRAC 6665 and 6675 Focused SOAP Note ExemplarDocumento6 pagineNRNP PRAC 6665 and 6675 Focused SOAP Note ExemplarLogan ZaraNessuna valutazione finora
- Anglo Afghan WarsDocumento79 pagineAnglo Afghan WarsNisar AhmadNessuna valutazione finora
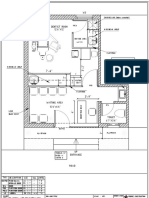
- Dental Clinic - Floor Plan R3-2Documento1 paginaDental Clinic - Floor Plan R3-2kanagarajodisha100% (1)
- The Future Mixed TensesDocumento4 pagineThe Future Mixed TensesChernykh Vitaliy100% (1)
- Limited Alembic: Employee Related DataDocumento4 pagineLimited Alembic: Employee Related DataTp EarningsNessuna valutazione finora
- Thesis Statement On Lionel MessiDocumento4 pagineThesis Statement On Lionel Messidwham6h1100% (2)
- Dial 1298 For Ambulance - HSBCDocumento22 pagineDial 1298 For Ambulance - HSBCDial1298forAmbulanceNessuna valutazione finora
- EVS (Yuva)Documento88 pagineEVS (Yuva)dasbaldev73Nessuna valutazione finora
- Directorate of Indian Medicines & Homoeopathy, Orissa, Bhubaneswar Listof The Homoeopathic Dispensaries BhadrakDocumento1 paginaDirectorate of Indian Medicines & Homoeopathy, Orissa, Bhubaneswar Listof The Homoeopathic Dispensaries Bhadrakbiswajit mathematicsNessuna valutazione finora
- Auditing Theory Auditing in A Computer Information Systems (Cis) EnvironmentDocumento32 pagineAuditing Theory Auditing in A Computer Information Systems (Cis) EnvironmentMajoy BantocNessuna valutazione finora
- IBM Thinkpad Z61 Quanta BW2Documento80 pagineIBM Thinkpad Z61 Quanta BW2Abubakar SidikNessuna valutazione finora
- Substitution Reactions - PMDocumento64 pagineSubstitution Reactions - PMprasoon jhaNessuna valutazione finora
- Module 8 - Emotional Intelligence Personal DevelopmentDocumento19 pagineModule 8 - Emotional Intelligence Personal DevelopmentRoxan Binarao-Bayot60% (5)
- Chapter 17 Study Guide: VideoDocumento7 pagineChapter 17 Study Guide: VideoMruffy DaysNessuna valutazione finora
- MVC Training Course Prerequisite: WWW - Focustech.InDocumento2 pagineMVC Training Course Prerequisite: WWW - Focustech.InLakshman Samanth ReddyNessuna valutazione finora