Potrebbero piacerti anche
- Architecture For Psychiatric EnvironmentDocumento193 pagineArchitecture For Psychiatric Environmentserena KazokuNessuna valutazione finora
- Hospital Outdoor Spaces - Therapeutic Benefits and Design ConsiderationsDocumento15 pagineHospital Outdoor Spaces - Therapeutic Benefits and Design Considerationsmimk2014Nessuna valutazione finora
- To Study Modern Hospice Designs:The Architecture of Palliative Care and HealingDocumento4 pagineTo Study Modern Hospice Designs:The Architecture of Palliative Care and HealingPRACHI MANTRI100% (1)
- Mental Health Facilities Design GuideDocumento317 pagineMental Health Facilities Design GuideIDrHotdog100% (1)
- Foreign-Architecture For Psychiatric TreatmentDocumento69 pagineForeign-Architecture For Psychiatric Treatmentchester fabic0% (1)
- Stressed Spaces - Mental Health and ArchitectureDocumento44 pagineStressed Spaces - Mental Health and ArchitectureMara BujorNessuna valutazione finora
- Effects of Healthcare Environmental Design On Medical Outcomes PDFDocumento11 pagineEffects of Healthcare Environmental Design On Medical Outcomes PDFAgnes Cheverloo Castillo100% (1)
- Healing Architecture Daylight in Hospital Design-LibreDocumento9 pagineHealing Architecture Daylight in Hospital Design-LibreAdita RianNessuna valutazione finora
- Alan Dilani WCDH2003Documento11 pagineAlan Dilani WCDH2003Muhamad RatodiNessuna valutazione finora
- Design For Mental and Behavioral Health 2017Documento283 pagineDesign For Mental and Behavioral Health 2017Ana EclipseNessuna valutazione finora
- Architecture in Theraupetic EnvironmentsDocumento27 pagineArchitecture in Theraupetic EnvironmentsJoshua RevanthNessuna valutazione finora
- Stressed Spaces PDFDocumento43 pagineStressed Spaces PDFKarla CarrascoNessuna valutazione finora
- Preventing Psychological Disorders in Service Members and Their Families An Assessment of ProgramsDocumento293 paginePreventing Psychological Disorders in Service Members and Their Families An Assessment of ProgramsFrancisco Guedes FilhoNessuna valutazione finora
- Healing ArchitectureDocumento16 pagineHealing ArchitectureZoona JerralNessuna valutazione finora
- Healing Architecture Daysdlight in Hospital DesignDocumento9 pagineHealing Architecture Daysdlight in Hospital DesignHealthene Joy Familara Alesna100% (1)
- Environmental Effects On HealingDocumento7 pagineEnvironmental Effects On Healingapi-514394058Nessuna valutazione finora
- The Psychological Impact of Architectural DesignDocumento44 pagineThe Psychological Impact of Architectural DesignmaygracedigolNessuna valutazione finora
- Architectural HealingDocumento20 pagineArchitectural HealingAarzan Vajracharya100% (1)
- Healing Environment PDFDocumento4 pagineHealing Environment PDFPraba KaranNessuna valutazione finora
- Drug Rehabitation Center SynopsisDocumento6 pagineDrug Rehabitation Center SynopsisPriya Dharshini Pd100% (1)
- Salutogenesis in Healthcare SettingsDocumento10 pagineSalutogenesis in Healthcare SettingsGulienne Randee Mickhaela ZamoraNessuna valutazione finora
- Vermont Psychiatric Care HospitalDocumento16 pagineVermont Psychiatric Care HospitalEsayase Asnake100% (1)
- Architectural Academic ThesisDocumento11 pagineArchitectural Academic ThesisYeong Kam LoongNessuna valutazione finora
- Health Psychology: Dr. Rosalyn M. King, ProfessorDocumento43 pagineHealth Psychology: Dr. Rosalyn M. King, ProfessorFasihah LiewNessuna valutazione finora
- Architectural Healing EnvironmentsDocumento90 pagineArchitectural Healing Environmentssakthivisalakshi83% (6)
- What Are Healing GardensDocumento9 pagineWhat Are Healing GardensMuhammad Tahir PervaizNessuna valutazione finora
- Healing Through BiophilicDocumento4 pagineHealing Through BiophilicMOHAMMAD SIDDIQ SALIMNessuna valutazione finora
- Therapeutic ArchitectureDocumento28 pagineTherapeutic ArchitectureKushalKumar50% (2)
- Rehab CenterDocumento15 pagineRehab CenterRaul Andrei MiuNessuna valutazione finora
- Addressing Sexual Assault - How Architectural Design Can Promote LDocumento94 pagineAddressing Sexual Assault - How Architectural Design Can Promote Lwefor youNessuna valutazione finora
- Dissertation On Healing Architecture in Hospital DesignDocumento114 pagineDissertation On Healing Architecture in Hospital DesignDipesh Anand86% (44)
- A Texas Hospital - Center For Sustainable DevelopmentDocumento180 pagineA Texas Hospital - Center For Sustainable Developmentdean j almy III100% (1)
- Hospice Care Resort: Pre-Oral DefenseDocumento37 pagineHospice Care Resort: Pre-Oral DefenseHoney Apruebo BascosNessuna valutazione finora
- Synopsis of Psychiatric HospitalDocumento8 pagineSynopsis of Psychiatric HospitalAATIF SHAIKHNessuna valutazione finora
- Chapter 1 Thesis SampleDocumento13 pagineChapter 1 Thesis SampleMarkAguilozNessuna valutazione finora
- Healing Pathways Thesis Book PDFDocumento106 pagineHealing Pathways Thesis Book PDFPraba Karan100% (1)
- Community Psychiatry Gp5Documento34 pagineCommunity Psychiatry Gp5Codillia CheongNessuna valutazione finora
- An Integrated Review of Evidence-Based Healthcare Design For Healing Environments Focusing On Longterm Care FacilitiesDocumento16 pagineAn Integrated Review of Evidence-Based Healthcare Design For Healing Environments Focusing On Longterm Care FacilitiesAmira EsamNessuna valutazione finora
- Healing EnviromentDocumento11 pagineHealing EnviromentAmol HopeNessuna valutazione finora
- Outpatients Unit - Guideline Section - International Health Facility GuidelinesDocumento23 pagineOutpatients Unit - Guideline Section - International Health Facility GuidelinesSebastian laierNessuna valutazione finora
- 1# Architectural Psychology: The Influence of Architecture On Our PsycheDocumento12 pagine1# Architectural Psychology: The Influence of Architecture On Our PsycheAnand JebasinghNessuna valutazione finora
- Psychology in Cancer HospitalDocumento28 paginePsychology in Cancer HospitalHimanshu Tripathi100% (1)
- RIAAADocumento9 pagineRIAAASakshi AjmeraNessuna valutazione finora
- Healing Through ArchitectureDocumento4 pagineHealing Through ArchitectureShivani Tandon100% (1)
- Hospital Interior Designing Services PDFDocumento6 pagineHospital Interior Designing Services PDFreddi.demullu007Nessuna valutazione finora
- Psychology and Architecture PDFDocumento5 paginePsychology and Architecture PDFZahid EmuNessuna valutazione finora
- Biophilic DesignDocumento2 pagineBiophilic DesignTriana RahayuNessuna valutazione finora
- Effect of Applying Therapeutic Architect PDFDocumento7 pagineEffect of Applying Therapeutic Architect PDFSandra MosesNessuna valutazione finora
- ROLE OF COLOURS IN Palliative Research PaperDocumento26 pagineROLE OF COLOURS IN Palliative Research PaperPriyank PatelNessuna valutazione finora
- Healing ArchitectureDocumento6 pagineHealing Architecturegrandnm100% (4)
- Evidence Based Healthcare DesignDocumento66 pagineEvidence Based Healthcare DesignGerry C FinneyNessuna valutazione finora
- Healing Through Architecture in Psychiatric HospitalsDocumento17 pagineHealing Through Architecture in Psychiatric HospitalsNidhi KrishnaswamyNessuna valutazione finora
- Healing Architecture Final ReportDocumento35 pagineHealing Architecture Final ReportAlisha PradhanNessuna valutazione finora
- Integrating Architectural Design To The Clinical Areas of The Hospital PDFDocumento137 pagineIntegrating Architectural Design To The Clinical Areas of The Hospital PDFJOSEPH APPIAH100% (1)
- Rehabilitation and ArchitectureDocumento2 pagineRehabilitation and ArchitecturePratap FaujdarNessuna valutazione finora
- Biophilic DesignDocumento6 pagineBiophilic DesignSamuel Zara100% (1)
- Healing HospitalDocumento48 pagineHealing HospitalNur Laela100% (1)
- Dilani, A. Design and HealthDocumento181 pagineDilani, A. Design and HealthCatarina FreitasNessuna valutazione finora
- Healing ArchitectureDocumento5 pagineHealing ArchitectureSUDHAKARMANI100% (2)
- Distributing Health Care: Principles, Practices and PoliticsDa EverandDistributing Health Care: Principles, Practices and PoliticsNessuna valutazione finora
- (Psychology of Emotions, Motivations and Actions) David A. Contreras-Psychology of Thinking (Psychology of Emotions, Motivations and Actions) - Nova Science Pub Inc (2010)Documento196 pagine(Psychology of Emotions, Motivations and Actions) David A. Contreras-Psychology of Thinking (Psychology of Emotions, Motivations and Actions) - Nova Science Pub Inc (2010)Drew AndersonNessuna valutazione finora
- BoConcept Interior Design Magazine - 2006-2007Documento188 pagineBoConcept Interior Design Magazine - 2006-2007IDrHotdogNessuna valutazione finora
- Assemble: Desk System List Price and Specification Guide V 13.9Documento16 pagineAssemble: Desk System List Price and Specification Guide V 13.9IDrHotdogNessuna valutazione finora
- Isku CatalogueDocumento28 pagineIsku CatalogueIDrHotdogNessuna valutazione finora
- Doors & WindowsDocumento6 pagineDoors & WindowsIDrHotdogNessuna valutazione finora
- 3DS Max Tutorial - The User InterfaceDocumento10 pagine3DS Max Tutorial - The User InterfaceIDrHotdogNessuna valutazione finora
- VK3021 Quick Response Pendent Sprinkler K5.6 (80.6) : 1. Product IdentificationDocumento19 pagineVK3021 Quick Response Pendent Sprinkler K5.6 (80.6) : 1. Product Identificationwika mepNessuna valutazione finora
- Kelebihan Triple StemcellDocumento4 pagineKelebihan Triple StemcellMuhammad AffandiNessuna valutazione finora
- Altronic Cpu-95 Ignition System Application List Medium Engines, 2-18 Cylinders FORM CPU-95 AL 1-02Documento11 pagineAltronic Cpu-95 Ignition System Application List Medium Engines, 2-18 Cylinders FORM CPU-95 AL 1-02dg_cd7340Nessuna valutazione finora
- Chapter 1-The Information System: An Accountant's PerspectiveDocumento20 pagineChapter 1-The Information System: An Accountant's PerspectiveJobby JaranillaNessuna valutazione finora
- General Biology 1: Quarter 1 - Module 1: Title: Cell TheoryDocumento19 pagineGeneral Biology 1: Quarter 1 - Module 1: Title: Cell TheoryAileen S. EncarnacionNessuna valutazione finora
- Pelicano Dalmata InstDocumento9 paginePelicano Dalmata InstEsteban NichoNessuna valutazione finora
- TAI PI 500 2018 FormattedDocumento54 pagineTAI PI 500 2018 FormattedShinoharaNessuna valutazione finora
- Beauty Imagined Jones en 14985Documento5 pagineBeauty Imagined Jones en 14985Internetian XNessuna valutazione finora
- Steel - WikipediaDocumento16 pagineSteel - WikipediaaravindNessuna valutazione finora
- Emilio Elizalde Et Al - Casimir Effect in de Sitter and Anti-De Sitter BraneworldsDocumento36 pagineEmilio Elizalde Et Al - Casimir Effect in de Sitter and Anti-De Sitter BraneworldsTurmav12345Nessuna valutazione finora
- Abc Stock AcquisitionDocumento13 pagineAbc Stock AcquisitionMary Joy AlbandiaNessuna valutazione finora
- Bridge Bearing & Expamnsion Joints PDFDocumento222 pagineBridge Bearing & Expamnsion Joints PDFmekkawi665086% (7)
- ITN 7.02 - Case Study - Part 1 (Modules 1-3)Documento2 pagineITN 7.02 - Case Study - Part 1 (Modules 1-3)tssr15.nadjemNessuna valutazione finora
- Global Supply Chain M11207Documento4 pagineGlobal Supply Chain M11207Anonymous VVSLkDOAC133% (3)
- NSN Form 2013 PDFDocumento136 pagineNSN Form 2013 PDFAnca IacobNessuna valutazione finora
- Algebra 2 Quarter 3 Do NowsDocumento50 pagineAlgebra 2 Quarter 3 Do Nowsapi-214128188Nessuna valutazione finora
- 2 6 7 HypervolemiaDocumento4 pagine2 6 7 HypervolemiaMaica LectanaNessuna valutazione finora
- Chemical Spillage Training 2024Documento30 pagineChemical Spillage Training 2024Sreedharan KannanNessuna valutazione finora
- Seminar TopicsDocumento21 pagineSeminar Topics123321Nessuna valutazione finora
- TakeoversDocumento10 pagineTakeoversCuong Huy NguyenNessuna valutazione finora
- Slag - WikipediaDocumento15 pagineSlag - WikipediaHasan KamalNessuna valutazione finora
- North West Karnataka Road Transport Corporation: (Application For Student Bus Pass)Documento3 pagineNorth West Karnataka Road Transport Corporation: (Application For Student Bus Pass)RasoolkhanNessuna valutazione finora
- I Found The PathDocumento72 pagineI Found The PathmasterrkNessuna valutazione finora
- 1.1 IntroductionDocumento17 pagine1.1 IntroductionRicka ValinoNessuna valutazione finora
- Orgonium Orgone Energy ResearchDocumento37 pagineOrgonium Orgone Energy Researchlnln462ln100% (1)
- Dil 1232Documento18 pagineDil 1232iman alyahNessuna valutazione finora
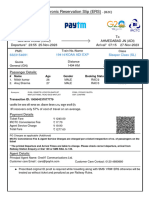
- Train TicketDocumento2 pagineTrain TicketSunil kumarNessuna valutazione finora
- Chapter 2 (Numerical) GarimaDocumento43 pagineChapter 2 (Numerical) GarimaSudeep magarNessuna valutazione finora
- Dangerous Prohibited Goods Packaging Post GuideDocumento66 pagineDangerous Prohibited Goods Packaging Post Guidetonyd3Nessuna valutazione finora
- G Schock G-2210 ManualDocumento2 pagineG Schock G-2210 ManualcaquirinoNessuna valutazione finora