Potrebbero piacerti anche
- NCLEX-RN Exam Prep 2024-2025: 500 NCLEX-RN Test Prep Questions and Answers with ExplanationsDa EverandNCLEX-RN Exam Prep 2024-2025: 500 NCLEX-RN Test Prep Questions and Answers with ExplanationsNessuna valutazione finora
- Cvs (Diuretics)Documento2 pagineCvs (Diuretics)CatNessuna valutazione finora
- Drugs For AsthmaDocumento3 pagineDrugs For AsthmaMelissa Deso MillerNessuna valutazione finora
- Sarcoidosis: Dr. Col. Vishal MarwahaDocumento26 pagineSarcoidosis: Dr. Col. Vishal MarwahaSreekrishnan TrikkurNessuna valutazione finora
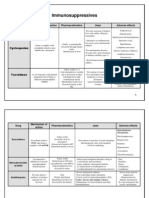
- 1 - Immuno Tables1Documento4 pagine1 - Immuno Tables1Urugonda VenumadhavNessuna valutazione finora
- Mental Status Examination Medical StudentsDocumento23 pagineMental Status Examination Medical StudentseurocoupeNessuna valutazione finora
- Family Medicine OSCE Dr. Rebeca HoilettDocumento20 pagineFamily Medicine OSCE Dr. Rebeca HoilettFatma El FaresNessuna valutazione finora
- Asthma DrugsDocumento1 paginaAsthma DrugskakuNessuna valutazione finora
- FMS 1 - Week 7 Tutorial 1 LO PDFDocumento17 pagineFMS 1 - Week 7 Tutorial 1 LO PDFAprillia AlmaasNessuna valutazione finora
- Case Studies On Major Concepts: OxygenationDocumento37 pagineCase Studies On Major Concepts: OxygenationJek Dela CruzNessuna valutazione finora
- Hematologic DisordersDocumento32 pagineHematologic DisordersQuolette ConstanteNessuna valutazione finora
- Week-2 Mental Status ExaminationDocumento23 pagineWeek-2 Mental Status ExaminationSaud TariqNessuna valutazione finora
- Antiepileptic DrugsDocumento65 pagineAntiepileptic DrugsZarish IftikharNessuna valutazione finora
- Case History M.SCDocumento10 pagineCase History M.SCRaksha RNNessuna valutazione finora
- Respiratory AssessmentDocumento43 pagineRespiratory AssessmentLui Andrei AnilaNessuna valutazione finora
- Description of The Patient & Instructions To SimulatorDocumento7 pagineDescription of The Patient & Instructions To SimulatorCindy WongNessuna valutazione finora
- 3-Major Veins of The BodyDocumento26 pagine3-Major Veins of The BodyTJPlayz100% (1)
- Medical Boards Step 2 Made Ridiculously Simple (Medicalstudyzone - Com)Documento377 pagineMedical Boards Step 2 Made Ridiculously Simple (Medicalstudyzone - Com)Benyamin KhalevNessuna valutazione finora
- Anatomy and Physiology of PlacentaDocumento5 pagineAnatomy and Physiology of PlacentaAmuNessuna valutazione finora
- ECG Demographics Rate: 300/# Large Box in RR IntervalDocumento11 pagineECG Demographics Rate: 300/# Large Box in RR IntervalJonathan DavisNessuna valutazione finora
- Anti Viral DrugsDocumento6 pagineAnti Viral DrugskakuNessuna valutazione finora
- Immune System Docs 2019Documento13 pagineImmune System Docs 2019David DavidNessuna valutazione finora
- Transfusion For ChildrenDocumento5 pagineTransfusion For ChildrenKristine Mae AbrasaldoNessuna valutazione finora
- 7th Edition All NeuroDocumento92 pagine7th Edition All NeuroCrystal LynaeNessuna valutazione finora
- IV Fluid ChartDocumento2 pagineIV Fluid Chartbenny christantoNessuna valutazione finora
- Pneumonia: 1. Pleural Effusion 3. Septic ShockDocumento1 paginaPneumonia: 1. Pleural Effusion 3. Septic ShockTrisha VergaraNessuna valutazione finora
- Chest Pain Chest Pain: Focused History Focused Physical ExamDocumento1 paginaChest Pain Chest Pain: Focused History Focused Physical ExamdocNessuna valutazione finora
- Hem-Onc: AnswerDocumento3 pagineHem-Onc: AnswerAman Raj KNessuna valutazione finora
- Medicine OSCE - Common Diseases Ver2Documento4 pagineMedicine OSCE - Common Diseases Ver2TrisNessuna valutazione finora
- Pain 2. Pallor Poikylothermia Parasthesia Pulselessness Factor V Leiden (Activated Protein C Resistance)Documento3 paginePain 2. Pallor Poikylothermia Parasthesia Pulselessness Factor V Leiden (Activated Protein C Resistance)Ryan TurnerNessuna valutazione finora
- Drugs For Heart Failure: Drugs Catego Ry Drug Function Adverse Effect NoteDocumento2 pagineDrugs For Heart Failure: Drugs Catego Ry Drug Function Adverse Effect NoteyukariNessuna valutazione finora
- Antihypotensive Drugs: Roger Joseph Ii Ramos Jecino, RN, M.DDocumento28 pagineAntihypotensive Drugs: Roger Joseph Ii Ramos Jecino, RN, M.DFranz Earl Niño AlbesaNessuna valutazione finora
- Endocrine DisordersDocumento5 pagineEndocrine DisordersBilly Ray VillanuevaNessuna valutazione finora
- Autoimmune Diseases: Henry O. Ogedegbe, PHD., C (Ascp) SC Department of EhmcsDocumento47 pagineAutoimmune Diseases: Henry O. Ogedegbe, PHD., C (Ascp) SC Department of EhmcsGalih Putra RanggaNessuna valutazione finora
- Female Reproductive Ogans Internal Organs of ReproductionDocumento22 pagineFemale Reproductive Ogans Internal Organs of ReproductionAngela NeriNessuna valutazione finora
- 50 Most Commonly Prescribed MedicationsDocumento2 pagine50 Most Commonly Prescribed Medications1stsgtwife4055Nessuna valutazione finora
- 2a Haematology Saq QuestionsDocumento12 pagine2a Haematology Saq QuestionskamaluNessuna valutazione finora
- Diuretic DrugsDocumento2 pagineDiuretic DrugsEngku ElisaNessuna valutazione finora
- Pharmacology - Use of Beta-Blockers & Arbs in Cardiovascular Disease Treating HypertensionDocumento5 paginePharmacology - Use of Beta-Blockers & Arbs in Cardiovascular Disease Treating HypertensionDana20SNessuna valutazione finora
- GI Signs and SymptomsDocumento40 pagineGI Signs and SymptomsJohnny BeeNessuna valutazione finora
- 4 Blood ProductsDocumento11 pagine4 Blood ProductsGampa VijaykumarNessuna valutazione finora
- Immune System Review QuestionsDocumento2 pagineImmune System Review Questionsapi-524061079Nessuna valutazione finora
- Assessment and Management of Patients With Biliary DisorderDocumento50 pagineAssessment and Management of Patients With Biliary DisorderZanida ZainonNessuna valutazione finora
- 1-Adrenocorticosteroids Chapter39Documento94 pagine1-Adrenocorticosteroids Chapter39hamidNessuna valutazione finora
- Immunopharmacology: Dr. Hamad AlshabiDocumento8 pagineImmunopharmacology: Dr. Hamad AlshabiHamad Alshabi100% (1)
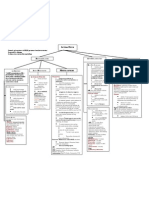
- Concept Map Week 2Documento2 pagineConcept Map Week 2Ashley ChristensenNessuna valutazione finora
- Sympathomimetic Agents: CLIN. PHARM (Dr. Salvador) Asthma 05 SEPT 2017Documento3 pagineSympathomimetic Agents: CLIN. PHARM (Dr. Salvador) Asthma 05 SEPT 2017Seff Causapin100% (1)
- Valvular Heart DseDocumento8 pagineValvular Heart DseJane Pineda CuraNessuna valutazione finora
- Abdominal Swelling + AscitesDocumento29 pagineAbdominal Swelling + AscitesDevina CiayadiNessuna valutazione finora
- Disease & Def Patho/Mech Clinical S/S DX/ Tests/Labs TX NotesDocumento11 pagineDisease & Def Patho/Mech Clinical S/S DX/ Tests/Labs TX NotesSara AshurstNessuna valutazione finora
- Approach To Unconscious PatientDocumento23 pagineApproach To Unconscious Patienttantw880% (1)
- Anatomy Ospe PDFDocumento25 pagineAnatomy Ospe PDFrizki ardiansyahNessuna valutazione finora
- Nephrotic and NephriticDocumento27 pagineNephrotic and Nephritictam meiNessuna valutazione finora
- Internal Medicine VivasDocumento9 pagineInternal Medicine Vivasponcus payNessuna valutazione finora
- Pharma GI CardsDocumento16 paginePharma GI CardsDoctorsHangout.comNessuna valutazione finora
- Disoreder of PerceptionDocumento36 pagineDisoreder of PerceptionUmar Khan100% (1)
- Self-Bullying: What to do when the bully is YOU!Da EverandSelf-Bullying: What to do when the bully is YOU!Nessuna valutazione finora
- Optimal Life: Essentials of AsthmaDa EverandOptimal Life: Essentials of AsthmaNessuna valutazione finora
- FIrstAidCLerkship EM DiagnosticsDocumento3 pagineFIrstAidCLerkship EM DiagnosticscrystalsheNessuna valutazione finora
- OSCE Stop - Lecture Long HistoryDocumento18 pagineOSCE Stop - Lecture Long HistorycrystalsheNessuna valutazione finora
- Lange Current Emergency Medicine - GI Bleed ChapterDocumento3 pagineLange Current Emergency Medicine - GI Bleed ChaptercrystalsheNessuna valutazione finora
- ACLS Provider Manual 2015 NotesDocumento5 pagineACLS Provider Manual 2015 Notescrystalshe93% (14)
- Packrat Cardio QuestionsDocumento63 paginePackrat Cardio Questionscrystalshe100% (1)
- Bates Thorax Lungs With TermsDocumento4 pagineBates Thorax Lungs With Termscrystalshe100% (1)
- Pathophysiology LymphomaDocumento4 paginePathophysiology LymphomacrystalsheNessuna valutazione finora
- Adjuncts Quiz 1: Study Online atDocumento5 pagineAdjuncts Quiz 1: Study Online atcrystalsheNessuna valutazione finora
- Quick Facts For Electrolyte AnalysisDocumento3 pagineQuick Facts For Electrolyte AnalysiscrystalsheNessuna valutazione finora
- Head Neck Infections Obstructive Airway Disease FactsDocumento17 pagineHead Neck Infections Obstructive Airway Disease FactscrystalsheNessuna valutazione finora
- Kidneys Fluid Regulation ElectrolytesDocumento10 pagineKidneys Fluid Regulation Electrolytescrystalshe100% (1)
- DRUG STUDY-1st BatchDocumento27 pagineDRUG STUDY-1st BatchCanny CańasNessuna valutazione finora
- Cardiac Output: Prof. K. SivapalanDocumento9 pagineCardiac Output: Prof. K. SivapalanjikookNessuna valutazione finora
- Health 8Documento319 pagineHealth 8Anngela Arevalo BarcenasNessuna valutazione finora
- PDF TextDocumento3 paginePDF TextYogita PalNessuna valutazione finora
- Programme Guide Certificate in Community Health (BPCCHN) - CompressedDocumento120 pagineProgramme Guide Certificate in Community Health (BPCCHN) - CompressedChakrapani ChaturvediNessuna valutazione finora
- Week 4 Hand Washing and Ppe - CincoDocumento3 pagineWeek 4 Hand Washing and Ppe - CincoShecana Rose CincoNessuna valutazione finora
- Risk Assessments: What They Are, Why They're Important and How To Complete ThemDocumento5 pagineRisk Assessments: What They Are, Why They're Important and How To Complete ThemAL Hazm National ProjectsNessuna valutazione finora
- Aconitum Ferox - Blue AconiteDocumento2 pagineAconitum Ferox - Blue Aconitejcoppala4476100% (1)
- A Simplified List of All Protocols - HubermanLabDocumento2 pagineA Simplified List of All Protocols - HubermanLabMorten NessNessuna valutazione finora
- 5 Elements Qi GongDocumento1 pagina5 Elements Qi GongBill HonakerNessuna valutazione finora
- Hubungan Kejadian Dismenore Dengan Asupan Fe (Zat Besi) Pada Remaja PutriDocumento5 pagineHubungan Kejadian Dismenore Dengan Asupan Fe (Zat Besi) Pada Remaja Putriashar hariyantoNessuna valutazione finora
- 3.02 Medicina Clínica PDFDocumento100 pagine3.02 Medicina Clínica PDFCristina Maite Chacon AmayaNessuna valutazione finora
- Phoenix, Arizona: Principles To Guide Zoning For Community Residences For People With DisabilitiesDocumento44 paginePhoenix, Arizona: Principles To Guide Zoning For Community Residences For People With Disabilitiesdan-304518Nessuna valutazione finora
- Cyclo ThermDocumento24 pagineCyclo ThermProtantagonist91% (11)
- The Bethesda System For Reporting Cervical Cytolog PDFDocumento359 pagineThe Bethesda System For Reporting Cervical Cytolog PDFsurekhaNessuna valutazione finora
- Daftar Pustaka - 2pusssDocumento6 pagineDaftar Pustaka - 2pusssMuhammad ShodiqinNessuna valutazione finora
- NCERT Class 9 Political Science Chapter 6 YouTube Lecture HandoutsDocumento5 pagineNCERT Class 9 Political Science Chapter 6 YouTube Lecture Handoutsarjun anjana anjanaNessuna valutazione finora
- Acupuncture With Manual and Electrical Stimulation For Labour Pain: A Two Month Follow Up of Recollection of Pain and Birth ExperienceDocumento9 pagineAcupuncture With Manual and Electrical Stimulation For Labour Pain: A Two Month Follow Up of Recollection of Pain and Birth ExperiencejayaNessuna valutazione finora
- ICAO Manual Doc 9984 1st Edition Alltext en Published March 2013Documento54 pagineICAO Manual Doc 9984 1st Edition Alltext en Published March 2013Disability Rights Alliance67% (3)
- MSDS RBD Palm Olein cp10Documento4 pagineMSDS RBD Palm Olein cp10sugitra sawitaNessuna valutazione finora
- MRU-QMS-HSE-Form - JSA - Geotechnical Drilling & Geotechnical Field Investigation - Rev00Documento11 pagineMRU-QMS-HSE-Form - JSA - Geotechnical Drilling & Geotechnical Field Investigation - Rev00AditNessuna valutazione finora
- Nursing 2 4yDocumento10 pagineNursing 2 4yGCON KURNOOLNessuna valutazione finora
- Hypomochlion Aided Reduction For Sub-Condylar FracturesDocumento2 pagineHypomochlion Aided Reduction For Sub-Condylar FracturesshyamNessuna valutazione finora
- 02 Revman Exercise Caffeine Articles JournalsDocumento8 pagine02 Revman Exercise Caffeine Articles JournalsKenneth TorresNessuna valutazione finora
- Use of Mosquito Repellent Devices-Problems and Prospects: August 2018Documento6 pagineUse of Mosquito Repellent Devices-Problems and Prospects: August 2018Cyrus Ian LanuriasNessuna valutazione finora
- Carlton Hubbards ResumeDocumento2 pagineCarlton Hubbards Resumeapi-662079150Nessuna valutazione finora
- Effectiveness of An Anterior Mini-Screw in Achieving Incisor IntrusionDocumento10 pagineEffectiveness of An Anterior Mini-Screw in Achieving Incisor IntrusionAbdel Hadi KanjNessuna valutazione finora
- DHCDocumento2 pagineDHCLiaqat Ali KhanNessuna valutazione finora
- ISSLDocumento58 pagineISSLsufiNessuna valutazione finora
- AbDocumento5 pagineAbapi-466413302Nessuna valutazione finora