Potrebbero piacerti anche
- Social Norms Marketing Social Networks and Alcohol ConsumptionDocumento495 pagineSocial Norms Marketing Social Networks and Alcohol ConsumptionHappy IbiNessuna valutazione finora
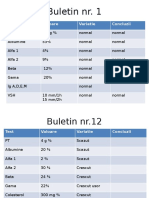
- Buletin Nr. 1: Test Valoare Variatie ConcluziiDocumento12 pagineBuletin Nr. 1: Test Valoare Variatie ConcluziiHappy IbiNessuna valutazione finora
- Rasp Farmaco Test 5Documento1 paginaRasp Farmaco Test 5Happy IbiNessuna valutazione finora
- NDocumento3 pagineNHappy IbiNessuna valutazione finora
- ANEXA 1 - Regulament Echivalare Stagiu ERASMUSDocumento1 paginaANEXA 1 - Regulament Echivalare Stagiu ERASMUSHappy IbiNessuna valutazione finora
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (400)
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (588)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (74)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (266)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (344)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (121)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- German Employment Visa Application: What Is A German Work Visa and Do I Need One?Documento4 pagineGerman Employment Visa Application: What Is A German Work Visa and Do I Need One?FarbodNessuna valutazione finora
- Computer Awareness: Special Edition E-BookDocumento54 pagineComputer Awareness: Special Edition E-BookTanujit SahaNessuna valutazione finora
- Affin Bank V Zulkifli - 2006Documento15 pagineAffin Bank V Zulkifli - 2006sheika_11Nessuna valutazione finora
- Puzzles 1Documento214 paginePuzzles 1Prince VegetaNessuna valutazione finora
- Morrison On Rarick (1966)Documento4 pagineMorrison On Rarick (1966)alex7878Nessuna valutazione finora
- King of Chess American English American English TeacherDocumento6 pagineKing of Chess American English American English TeacherJuliana FigueroaNessuna valutazione finora
- Gmail - Payment Received From Cnautotool - Com (Order No - Cnautot2020062813795)Documento2 pagineGmail - Payment Received From Cnautotool - Com (Order No - Cnautot2020062813795)Luis Gustavo Escobar MachadoNessuna valutazione finora
- Botswana Ref Ranges PaperDocumento7 pagineBotswana Ref Ranges PaperMunyaradzi MangwendezaNessuna valutazione finora
- A1 - The Canterville Ghost WorksheetsDocumento8 pagineA1 - The Canterville Ghost WorksheetsТатьяна ЩукинаNessuna valutazione finora
- Robbins FOM10ge C05Documento35 pagineRobbins FOM10ge C05Ahmed Mostafa ElmowafyNessuna valutazione finora
- Creole LanguagesDocumento2 pagineCreole LanguagesClaire AlexisNessuna valutazione finora
- Shaping School Culture Case StudyDocumento7 pagineShaping School Culture Case Studyapi-524477308Nessuna valutazione finora
- Chelsea Bellomy ResumeDocumento1 paginaChelsea Bellomy Resumeapi-301977181Nessuna valutazione finora
- Net 2020Documento48 pagineNet 2020Krishan pandeyNessuna valutazione finora
- Mse Return DemonstrationDocumento7 pagineMse Return DemonstrationMaggay LarsNessuna valutazione finora
- Practice For Those Who Are DyingDocumento10 paginePractice For Those Who Are DyingBecze István / Stephen Becze100% (1)
- SoapDocumento10 pagineSoapAira RamoresNessuna valutazione finora
- Portfolio Assignment MaternityDocumento2 paginePortfolio Assignment Maternityapi-319339803100% (1)
- Conflict Management and Negotiation - Team 5Documento34 pagineConflict Management and Negotiation - Team 5Austin IsaacNessuna valutazione finora
- Holistic Centre: Case Study 1 - Osho International Meditation Centre, Pune, IndiaDocumento4 pagineHolistic Centre: Case Study 1 - Osho International Meditation Centre, Pune, IndiaPriyesh Dubey100% (2)
- Vistas 1-7 Class - 12 Eng - NotesDocumento69 pagineVistas 1-7 Class - 12 Eng - Notesvinoth KumarNessuna valutazione finora
- Bar Waiter/waitress Duties and Responsibilities Step by Step Cruise Ship GuideDocumento6 pagineBar Waiter/waitress Duties and Responsibilities Step by Step Cruise Ship GuideAmahl CericoNessuna valutazione finora
- Singleton v. Cannizzaro FILED 10 17 17Documento62 pagineSingleton v. Cannizzaro FILED 10 17 17Monique Judge100% (1)
- CHAPTER 2-3 LipidDocumento20 pagineCHAPTER 2-3 LipidDaniel IsmailNessuna valutazione finora
- Yds Deneme Sinavi PDFDocumento16 pagineYds Deneme Sinavi PDFodysseyyyNessuna valutazione finora
- Robber Bridegroom Script 1 PDFDocumento110 pagineRobber Bridegroom Script 1 PDFRicardo GarciaNessuna valutazione finora
- Learning TheoryDocumento7 pagineLearning TheoryIMS AcadNessuna valutazione finora
- MKTG4471Documento9 pagineMKTG4471Aditya SetyaNessuna valutazione finora
- Excavations OSHA 2226Documento44 pagineExcavations OSHA 2226Al DubNessuna valutazione finora
- On Evil - Terry EagletonDocumento44 pagineOn Evil - Terry EagletonconelcaballocansadoNessuna valutazione finora