Potrebbero piacerti anche
- Revised National Tuberculosis Control Programme (RNTCP) : Dr. NavpreetDocumento30 pagineRevised National Tuberculosis Control Programme (RNTCP) : Dr. NavpreetYagnik SanjayNessuna valutazione finora
- RNTCPDocumento32 pagineRNTCPSuvendu Sekhar PandaNessuna valutazione finora
- National TB ControlDocumento25 pagineNational TB Controlnirmal2444Nessuna valutazione finora
- Overview of India's Revised National Tuberculosis Control ProgrammeDocumento65 pagineOverview of India's Revised National Tuberculosis Control Programmecatalyst1986100% (1)
- Revised National Tuberculosis Control Programme in IndiaDocumento25 pagineRevised National Tuberculosis Control Programme in IndiaSrilekha MaruthaiyanNessuna valutazione finora
- RNTCPDocumento24 pagineRNTCPmohanpskohli8310Nessuna valutazione finora
- Revised National Tuberculosis Control Programme (RNTCP) Milestones and AchievementsDocumento24 pagineRevised National Tuberculosis Control Programme (RNTCP) Milestones and Achievementsarunjv1234100% (1)
- NTEP or RNTCP (Community Health Nursing)Documento37 pagineNTEP or RNTCP (Community Health Nursing)Ankita ShaluNessuna valutazione finora
- Revised National Tuberculosis Control Program (RNTCP)Documento85 pagineRevised National Tuberculosis Control Program (RNTCP)Srilekha MaruthaiyanNessuna valutazione finora
- TB and Hiv/Aids: Care & Treatment UnitDocumento38 pagineTB and Hiv/Aids: Care & Treatment UnitAngga PahNessuna valutazione finora
- Revised National Tuberculosis Control Programme OverviewDocumento53 pagineRevised National Tuberculosis Control Programme Overviewarpitagupta28Nessuna valutazione finora
- RNTCP May 2007Documento44 pagineRNTCP May 2007Kadiri ReddeppaNessuna valutazione finora
- National Aids Control ProgDocumento45 pagineNational Aids Control ProgGirishkumar KrishnaNessuna valutazione finora
- Country Progress ReportDocumento19 pagineCountry Progress Reportprk1234Nessuna valutazione finora
- Tuberculosis: An OverviewDocumento45 pagineTuberculosis: An OverviewaNessuna valutazione finora
- TB ApDocumento117 pagineTB ApArun KumarNessuna valutazione finora
- TB Dots Module1Documento75 pagineTB Dots Module1Bryne Daniel Buya100% (1)
- TB and HIVDocumento62 pagineTB and HIVNational Press FoundationNessuna valutazione finora
- Revised National TB Control ProgramDocumento12 pagineRevised National TB Control ProgramsaurabhNessuna valutazione finora
- RNTCPDocumento20 pagineRNTCPSahil ShirkeNessuna valutazione finora
- Epidemiology Tuberculosis HODocumento46 pagineEpidemiology Tuberculosis HOHerman WaNessuna valutazione finora
- Prepared by Shanaz Marazi DPC Kupwara Under The Supervision of DTO Kupwara)Documento53 paginePrepared by Shanaz Marazi DPC Kupwara Under The Supervision of DTO Kupwara)Mir JavidNessuna valutazione finora
- Jurnal Diagnosis-1Documento6 pagineJurnal Diagnosis-1Dian ZiziNessuna valutazione finora
- Revised National Tuberculosis Control ProgrammeDocumento31 pagineRevised National Tuberculosis Control Programmeprincess 4100% (3)
- National Tuberculosis Control ProgramDocumento4 pagineNational Tuberculosis Control ProgramSlepy chngNessuna valutazione finora
- Gupta 2014Documento12 pagineGupta 2014Nguyen Nam AnhNessuna valutazione finora
- Identifying Gaps in The Quality of Latent Tuberculosis Infection CareDocumento5 pagineIdentifying Gaps in The Quality of Latent Tuberculosis Infection CareiboelkNessuna valutazione finora
- National AIDS Control ProgramDocumento29 pagineNational AIDS Control ProgramMonalisha SinghNessuna valutazione finora
- RNTCP - Wikipedia, The Free EncyclopediaDocumento5 pagineRNTCP - Wikipedia, The Free EncyclopediaakurilNessuna valutazione finora
- NHP 2Documento42 pagineNHP 2A J FathimaNessuna valutazione finora
- TB HIV Research Proposal HarishDocumento23 pagineTB HIV Research Proposal HarishLekha Bahadur Gurung100% (4)
- GLI AlgorithmsDocumento37 pagineGLI Algorithmssitharesmi Dien MangoendiharjoNessuna valutazione finora
- DOC-20240227-WA0004_##document##Documento12 pagineDOC-20240227-WA0004_##document##vinushakaveripakam26Nessuna valutazione finora
- National Aids Control ProgrammeDocumento77 pagineNational Aids Control Programmeangayarkanni100% (3)
- Pengendalian Dan Pencegahan Tuberkulosis: Diah HandayaniDocumento40 paginePengendalian Dan Pencegahan Tuberkulosis: Diah HandayanirudyfirNessuna valutazione finora
- NTEPDocumento18 pagineNTEP012 AKHILA SETHUNATHNessuna valutazione finora
- Publications - Through The CNS Lens - WHO Global TB Report 2012Documento16 paginePublications - Through The CNS Lens - WHO Global TB Report 2012bobbyramakantNessuna valutazione finora
- Materi Prof SoedarsonoDocumento36 pagineMateri Prof SoedarsonoSEKSI UKLWNessuna valutazione finora
- Tropicalmed 05 00026 v4Documento13 pagineTropicalmed 05 00026 v4D BasavarajaNessuna valutazione finora
- NTEP Organogram: India's Tuberculosis Control StructureDocumento18 pagineNTEP Organogram: India's Tuberculosis Control Structure012 AKHILA SETHUNATHNessuna valutazione finora
- TB PosterDocumento13 pagineTB Posterthamizhselvi87Nessuna valutazione finora
- Standard Manual For Laboratory Technicians On Sputum Smear MicrosDocumento67 pagineStandard Manual For Laboratory Technicians On Sputum Smear MicrosanisyaNessuna valutazione finora
- BCCDC TB ManualRevisedFebruary 2012Documento141 pagineBCCDC TB ManualRevisedFebruary 2012zenagit123456Nessuna valutazione finora
- 4 Epidemiology of TB and Management IssueDocumento35 pagine4 Epidemiology of TB and Management IssueAmisha MahajanNessuna valutazione finora
- What Is The Optimum Time To Start Antiretroviral Therapy in People With HIV and Tuberculosis Coinfection? A Systematic Review and Meta-AnalysisDocumento34 pagineWhat Is The Optimum Time To Start Antiretroviral Therapy in People With HIV and Tuberculosis Coinfection? A Systematic Review and Meta-Analysisbagir_dm10Nessuna valutazione finora
- National Aids Control ProgrammeDocumento12 pagineNational Aids Control ProgrammeNur Adilla MahmudNessuna valutazione finora
- National Viral Hepatitis Control Program - Reference File - 0Documento68 pagineNational Viral Hepatitis Control Program - Reference File - 0SSNessuna valutazione finora
- Thesis PDFDocumento46 pagineThesis PDFShariqNessuna valutazione finora
- Presentation Intro TuberculosisDocumento8 paginePresentation Intro TuberculosisEidi IdhamNessuna valutazione finora
- Revised National Tuberculosis Control ProgrammeDocumento7 pagineRevised National Tuberculosis Control Programmescribd1Nessuna valutazione finora
- Newer Diagnostic Tests For Tuberculosis Their UtilDocumento5 pagineNewer Diagnostic Tests For Tuberculosis Their UtilAbrar TaraNessuna valutazione finora
- Diagnostics Xpert MTB/RIF Test: Who RecommendationsDocumento2 pagineDiagnostics Xpert MTB/RIF Test: Who Recommendationsfreddy fitriadyNessuna valutazione finora
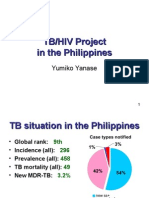
- TB/HIV Project in PhilippinesDocumento22 pagineTB/HIV Project in PhilippinesJohnryl FranciscoNessuna valutazione finora
- Burden and Consequences of Tuberculosis Among HIV-Infected Individuals Insights From The Itojo Hospital HIV Clinic in Ntungamo DistrictDocumento8 pagineBurden and Consequences of Tuberculosis Among HIV-Infected Individuals Insights From The Itojo Hospital HIV Clinic in Ntungamo DistrictKIU PUBLICATION AND EXTENSIONNessuna valutazione finora
- Synopsis Frequency of Non-Adherence To Previous Treatment in Relapse Tuberculosis PatientsDocumento5 pagineSynopsis Frequency of Non-Adherence To Previous Treatment in Relapse Tuberculosis PatientsAneesUrRahmanNessuna valutazione finora
- TB and HIVDocumento43 pagineTB and HIVNational Press Foundation100% (1)
- Presentation 1: - Global Tuberculosis Scenario - RNTCP-Evolution, Objectives, Structure, AchievementsDocumento26 paginePresentation 1: - Global Tuberculosis Scenario - RNTCP-Evolution, Objectives, Structure, AchievementsShiddappa MadarNessuna valutazione finora
- Prevalence of Human Immunodeficiency Virus Infection Among Tuberculosis Patients at Infectious Disease Hospital, Kano State, NigeriaDocumento8 paginePrevalence of Human Immunodeficiency Virus Infection Among Tuberculosis Patients at Infectious Disease Hospital, Kano State, NigeriaUMYU Journal of Microbiology Research (UJMR)Nessuna valutazione finora
- National Tuberculosis Control Program: Dr. Kanupriya ChaturvediDocumento37 pagineNational Tuberculosis Control Program: Dr. Kanupriya ChaturvediBen JosephNessuna valutazione finora
- SARS-CoV-2 Viral Outbreak Investigation: Laboratory Perspective: Clinical Updates in COVID-19Da EverandSARS-CoV-2 Viral Outbreak Investigation: Laboratory Perspective: Clinical Updates in COVID-19Valutazione: 3 su 5 stelle3/5 (1)
- Ashoknagar PopulationDocumento2 pagineAshoknagar PopulationDeepa SharmaNessuna valutazione finora
- Electrophoresis 4Documento19 pagineElectrophoresis 4Deepa SharmaNessuna valutazione finora
- Air PollutionDocumento15 pagineAir PollutionDeepa SharmaNessuna valutazione finora
- Alphabetical List of Towns and Their Population: Madhya PradeshDocumento14 pagineAlphabetical List of Towns and Their Population: Madhya PradeshDeepa SharmaNessuna valutazione finora
- Frank GeryDocumento19 pagineFrank GeryDeepa SharmaNessuna valutazione finora
- Guidelines Quarterly ANCDRDocumento3 pagineGuidelines Quarterly ANCDRDeepa SharmaNessuna valutazione finora
- 20 Artists Who Took Embroidery To The Next Level - Bored PandaDocumento47 pagine20 Artists Who Took Embroidery To The Next Level - Bored PandaDeepa SharmaNessuna valutazione finora
- Criteria For Hazardous Waste Landfills PDFDocumento54 pagineCriteria For Hazardous Waste Landfills PDFDeepa SharmaNessuna valutazione finora
- Placemaking: Sense of Place in Urban SpacesDocumento3 paginePlacemaking: Sense of Place in Urban SpacesDeepa SharmaNessuna valutazione finora
- Bufeb 02Documento7 pagineBufeb 02Deepa SharmaNessuna valutazione finora
- Second Professional M.B.B.S. (Annual), 2015 (Uploaded On 1st January, 2016)Documento31 pagineSecond Professional M.B.B.S. (Annual), 2015 (Uploaded On 1st January, 2016)Deepa SharmaNessuna valutazione finora
- Bharat B HwanDocumento16 pagineBharat B HwanDeepa Sharma50% (2)
- 32 Stylish Outdoor Planters To Perk Up Your Garden or Patio Photos - Architectural DigestDocumento34 pagine32 Stylish Outdoor Planters To Perk Up Your Garden or Patio Photos - Architectural DigestDeepa SharmaNessuna valutazione finora
- Elektroforesis HemoglobinDocumento4 pagineElektroforesis HemoglobinElvan Dwi WidyadiNessuna valutazione finora
- Technical & Operational Guidelines For TB ControlDocumento154 pagineTechnical & Operational Guidelines For TB ControlDeepa SharmaNessuna valutazione finora
- Hemoglobinopathy Sarah WalterDocumento46 pagineHemoglobinopathy Sarah WalterDeepa SharmaNessuna valutazione finora
- Gothic, Byzantine ArchitectureDocumento26 pagineGothic, Byzantine ArchitectureDeepa SharmaNessuna valutazione finora
- Acoustical Ceilings and FloorsDocumento17 pagineAcoustical Ceilings and FloorsDeepa SharmaNessuna valutazione finora
- Precast ConcreteDocumento20 paginePrecast ConcreteDeepa SharmaNessuna valutazione finora
- Human Psychology and Architecture DeepaDocumento15 pagineHuman Psychology and Architecture DeepaDeepa SharmaNessuna valutazione finora
- Diff. Types of RoofsDocumento16 pagineDiff. Types of RoofsDeepa SharmaNessuna valutazione finora
- Charles Correa's Architectural Masterpiece - Bharat Bhavan Art Centre in BhopalDocumento21 pagineCharles Correa's Architectural Masterpiece - Bharat Bhavan Art Centre in BhopalDeepa Sharma67% (12)
- Structural Analysis of Al-Burj DubaiDocumento15 pagineStructural Analysis of Al-Burj DubaiDeepa Sharma100% (1)
- Brindavan Garden: Submitted By: Deepa Sharma (101110047)Documento17 pagineBrindavan Garden: Submitted By: Deepa Sharma (101110047)Deepa Sharma40% (5)
- Handbook On Seismic Retrofit of Buildings - (Draft For Comments) - Apr2007Documento617 pagineHandbook On Seismic Retrofit of Buildings - (Draft For Comments) - Apr2007Nitin BehlNessuna valutazione finora
- Vertical Transportation Design and Elevator SelectionDocumento43 pagineVertical Transportation Design and Elevator SelectionGeet Jarvis Khurana100% (1)
- Majorda Beach Resort Goa GuideDocumento26 pagineMajorda Beach Resort Goa GuideDeepa SharmaNessuna valutazione finora
- Interior Design ReportDocumento22 pagineInterior Design ReportDeepa SharmaNessuna valutazione finora
- Urban Housing Scenario in Five Year PlansDocumento3 pagineUrban Housing Scenario in Five Year PlansDeepa SharmaNessuna valutazione finora
- Diagnostic Test - Pedia With Answer 50 Items Without RatioDocumento4 pagineDiagnostic Test - Pedia With Answer 50 Items Without RatioDennis Nabor Muñoz, RN,RMNessuna valutazione finora
- EveryDay AyurvedaDocumento11 pagineEveryDay AyurvedacvmraviNessuna valutazione finora
- Vocal Health and HygieneDocumento50 pagineVocal Health and HygieneclaugmailNessuna valutazione finora
- Adime Due 10 29Documento3 pagineAdime Due 10 29api-437192216Nessuna valutazione finora
- HTC Intake Form - September 4 - Final - Doc 7.9.13Documento10 pagineHTC Intake Form - September 4 - Final - Doc 7.9.13Kealeboga Duece ThoboloNessuna valutazione finora
- Ecg Quick Guide PDFDocumento7 pagineEcg Quick Guide PDFansarijavedNessuna valutazione finora
- Penjualan Total Juli 19Documento266 paginePenjualan Total Juli 19wartiniNessuna valutazione finora
- Pink Panther - Diabetes Management - Chapter 9Documento16 paginePink Panther - Diabetes Management - Chapter 9jennmoyerNessuna valutazione finora
- Final Benzodiazepine Guidelines Version 23 1495194854Documento18 pagineFinal Benzodiazepine Guidelines Version 23 1495194854Kru PrimeNessuna valutazione finora
- Try Out Paket BDocumento13 pagineTry Out Paket BDian Purnama Dp'TmNessuna valutazione finora
- MM M Hall of Femme Ebook 62463Documento15 pagineMM M Hall of Femme Ebook 62463Tayaba Naim KhanNessuna valutazione finora
- Aeromedical Transport TPDocumento8 pagineAeromedical Transport TPgalib20Nessuna valutazione finora
- BHP Formula No 55 Refrence - Bioplasgen 20 Homeopathic Medicine For Skin DiseasesDocumento2 pagineBHP Formula No 55 Refrence - Bioplasgen 20 Homeopathic Medicine For Skin DiseasesKazy Habibur RahmanNessuna valutazione finora
- Saudi Prometric Latest Questions AndanswerDocumento67 pagineSaudi Prometric Latest Questions AndanswerGloria Jaison100% (4)
- 12-Lead ECG Placement GuideDocumento9 pagine12-Lead ECG Placement GuideFalusi Blessing OlaideNessuna valutazione finora
- The Six-Step Formula for Hypnotic PersuasionDocumento24 pagineThe Six-Step Formula for Hypnotic Persuasionmajadb100% (12)
- Reasoning BookDocumento38 pagineReasoning BookAshish Sharma100% (1)
- Einstein's Theory of Relativity Explained Through His Life and CareerDocumento4 pagineEinstein's Theory of Relativity Explained Through His Life and Careeray2004jan29% (7)
- Kriya For Balancing The ChakrasDocumento5 pagineKriya For Balancing The ChakrasFedra Fox Cubeddu100% (2)
- Pediatric Voice PresentationDocumento16 paginePediatric Voice Presentationapi-254429093Nessuna valutazione finora
- Abdomen ExaminationDocumento37 pagineAbdomen ExaminationJaaydevNessuna valutazione finora
- Edna K.huffman - Health Information Managemen 1994Documento36 pagineEdna K.huffman - Health Information Managemen 1994gspot967% (6)
- 20 Uses of Vicks VaporubDocumento3 pagine20 Uses of Vicks VaporubDrBertram ForerNessuna valutazione finora
- Wiki Apgar Score01Documento3 pagineWiki Apgar Score01Leevon ThomasNessuna valutazione finora
- Circulatory SystemDocumento21 pagineCirculatory SystemKumar Sujeet100% (1)
- Negative Feedback Thyroxine and Adrenelin WsDocumento2 pagineNegative Feedback Thyroxine and Adrenelin WsEllie AbelNessuna valutazione finora
- Diet CounsellingDocumento11 pagineDiet CounsellingDrBhawna AroraNessuna valutazione finora
- Replacing ESR with Plasma ViscosityDocumento6 pagineReplacing ESR with Plasma ViscosityRyan ChenNessuna valutazione finora
- Disturbing Art Exposes Modern Culture AbsurditiesDocumento15 pagineDisturbing Art Exposes Modern Culture Absurdities2aethicusNessuna valutazione finora
- Notice Application Form For SRDocumento4 pagineNotice Application Form For SRPankaj PrasadNessuna valutazione finora