Potrebbero piacerti anche
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- History: Chief Complaint: History of Present Illness: Patient Is A 59 Year Old G6 P1051 Woman Who Is An Inmate That WasDocumento9 pagineHistory: Chief Complaint: History of Present Illness: Patient Is A 59 Year Old G6 P1051 Woman Who Is An Inmate That WasRoberto RamosNessuna valutazione finora
- Clinical CaseDocumento10 pagineClinical CaseRoberto RamosNessuna valutazione finora
- Case 2 AlmostDocumento8 pagineCase 2 AlmostRoberto RamosNessuna valutazione finora
- Case 3Documento8 pagineCase 3Roberto RamosNessuna valutazione finora
- Rhie Full OcrDocumento120 pagineRhie Full OcrRoberto RamosNessuna valutazione finora
- Case 4Documento8 pagineCase 4Roberto RamosNessuna valutazione finora
- Paciente 3Documento80 paginePaciente 3Roberto RamosNessuna valutazione finora
- Long Case Presentation FINAL-5Documento7 pagineLong Case Presentation FINAL-5Roberto RamosNessuna valutazione finora
- Universidad de Puerto Rico Mail - (No Subject)Documento77 pagineUniversidad de Puerto Rico Mail - (No Subject)Roberto RamosNessuna valutazione finora
- Long Case Presentation FINAL-5Documento7 pagineLong Case Presentation FINAL-5Roberto RamosNessuna valutazione finora
- Soap RoutineDocumento3 pagineSoap RoutineRoberto Ramos100% (1)
- There Is Been An Overlooked But Important TopicDocumento2 pagineThere Is Been An Overlooked But Important TopicRoberto RamosNessuna valutazione finora
- Repaso ShelfDocumento135 pagineRepaso ShelfRoberto RamosNessuna valutazione finora
- Long Case Presentation FINAL-33Documento7 pagineLong Case Presentation FINAL-33Roberto RamosNessuna valutazione finora
- Health Maintenance Cases For Discussion-5Documento4 pagineHealth Maintenance Cases For Discussion-5Roberto RamosNessuna valutazione finora
- "Repaso" Shelf OB - GYN 2 2Documento9 pagine"Repaso" Shelf OB - GYN 2 2Roberto RamosNessuna valutazione finora
- Radio ObGynDocumento1 paginaRadio ObGynRoberto RamosNessuna valutazione finora
- Progress Note Osce - HIV (1) - 2Documento1 paginaProgress Note Osce - HIV (1) - 2Roberto RamosNessuna valutazione finora
- Final - Answers of Ekg QuizDocumento46 pagineFinal - Answers of Ekg QuizRoberto RamosNessuna valutazione finora
- Untitled Spreadsheet 2Documento4 pagineUntitled Spreadsheet 2Roberto RamosNessuna valutazione finora
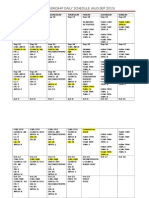
- Ob-Gyn Clerkship Daily Schedule (Aug-Sep 2015)Documento3 pagineOb-Gyn Clerkship Daily Schedule (Aug-Sep 2015)Roberto RamosNessuna valutazione finora
- DR - Umpierrere2012 2013 4Documento70 pagineDR - Umpierrere2012 2013 4Roberto RamosNessuna valutazione finora
- HTTPDocumento1 paginaHTTPRoberto RamosNessuna valutazione finora
- SEPSIS Case 2014 - August-2Documento45 pagineSEPSIS Case 2014 - August-2Roberto RamosNessuna valutazione finora
- Universidad Puerto Rico Manual 1415Documento161 pagineUniversidad Puerto Rico Manual 1415Roberto RamosNessuna valutazione finora
- There Is Been An Overlooked But Important TopicDocumento2 pagineThere Is Been An Overlooked But Important TopicRoberto RamosNessuna valutazione finora
- HTTPDocumento1 paginaHTTPRoberto RamosNessuna valutazione finora
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (344)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (399)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (588)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (73)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2259)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (120)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- Case Study McsDocumento4 pagineCase Study McsManjushree PatilNessuna valutazione finora
- A Detailed Lesson PlanDocumento5 pagineA Detailed Lesson PlanIsaac-elmar Agtarap74% (23)
- CH 1 Viscous Fluid Flow Part 1Documento29 pagineCH 1 Viscous Fluid Flow Part 1Ammar WahabNessuna valutazione finora
- Chapter 1 INTRODUCTION TO LITERATUREDocumento4 pagineChapter 1 INTRODUCTION TO LITERATUREDominique TurlaNessuna valutazione finora
- Democracy or Aristocracy?: Yasir MasoodDocumento4 pagineDemocracy or Aristocracy?: Yasir MasoodAjmal KhanNessuna valutazione finora
- XXXX96 01 01 2023to28 08 2023Documento18 pagineXXXX96 01 01 2023to28 08 2023dabu choudharyNessuna valutazione finora
- VTB Datasheet PDFDocumento24 pagineVTB Datasheet PDFNikola DulgiarovNessuna valutazione finora
- QF Jacket (Drafting & Cutting) - GAR620Documento15 pagineQF Jacket (Drafting & Cutting) - GAR620abdulraheem18822Nessuna valutazione finora
- DC Generator - Construction, Working Principle, Types, and Applications PDFDocumento1 paginaDC Generator - Construction, Working Principle, Types, and Applications PDFGokul GokulNessuna valutazione finora
- 3-A Y 3-B Brenda Franco DíazDocumento4 pagine3-A Y 3-B Brenda Franco DíazBRENDA FRANCO DIAZNessuna valutazione finora
- Charles Zastrow, Karen K. Kirst-Ashman-Understanding Human Behavior and The Social Environment-Thomson Brooks - Cole (2007)Documento441 pagineCharles Zastrow, Karen K. Kirst-Ashman-Understanding Human Behavior and The Social Environment-Thomson Brooks - Cole (2007)joan82% (17)
- Earth Science NAME - DATEDocumento3 pagineEarth Science NAME - DATEArlene CalataNessuna valutazione finora
- AVEVA LFM - Data Summary v2Documento6 pagineAVEVA LFM - Data Summary v2Joshua HobsonNessuna valutazione finora
- Present Perfect and Present Perfect ProgressiveDocumento5 paginePresent Perfect and Present Perfect ProgressiveKiara Fajardo matusNessuna valutazione finora
- STW 44 3 2 Model Course Leadership and Teamwork SecretariatDocumento49 pagineSTW 44 3 2 Model Course Leadership and Teamwork Secretariatwaranchai83% (6)
- Aman Singh Rathore Prelms Strategy For UPSCDocumento26 pagineAman Singh Rathore Prelms Strategy For UPSCNanju NNessuna valutazione finora
- Matutum View Academy: (The School of Faith)Documento14 pagineMatutum View Academy: (The School of Faith)Neil Trezley Sunico BalajadiaNessuna valutazione finora
- Unit 1 Building A Professional Relationship Across CulturesDocumento16 pagineUnit 1 Building A Professional Relationship Across CulturesAlex0% (1)
- Class InsectaDocumento4 pagineClass InsectaLittle Miss CeeNessuna valutazione finora
- PretestDocumento8 paginePretestAlmonte Aira LynNessuna valutazione finora
- Volcanoes Sub-topic:Volcanic EruptionDocumento16 pagineVolcanoes Sub-topic:Volcanic EruptionVhenz MapiliNessuna valutazione finora
- P D P: C I D, C M: Design of Coastal RoadsDocumento55 pagineP D P: C I D, C M: Design of Coastal RoadsMohammedNessuna valutazione finora
- Week 1 Familiarize The VmgoDocumento10 pagineWeek 1 Familiarize The VmgoHizzel De CastroNessuna valutazione finora
- SANDWICH Elisa (Procedure) - Immunology Virtual Lab I - Biotechnology and Biomedical Engineering - Amrita Vishwa Vidyapeetham Virtual LabDocumento2 pagineSANDWICH Elisa (Procedure) - Immunology Virtual Lab I - Biotechnology and Biomedical Engineering - Amrita Vishwa Vidyapeetham Virtual LabsantonuNessuna valutazione finora
- Effective TeachingDocumento94 pagineEffective Teaching小曼Nessuna valutazione finora
- Iso 22301 2019 en PDFDocumento11 pagineIso 22301 2019 en PDFImam Saleh100% (3)
- When SIBO & IBS-Constipation Are Just Unrecognized Thiamine DeficiencyDocumento3 pagineWhen SIBO & IBS-Constipation Are Just Unrecognized Thiamine Deficiencyps piasNessuna valutazione finora
- Oral Communication in ContextDocumento19 pagineOral Communication in ContextAzory ZelleNessuna valutazione finora
- DADTCO Presentation PDFDocumento34 pagineDADTCO Presentation PDFIngeniería Industrias Alimentarias Itsm100% (1)
- 1 AlarmvalveDocumento9 pagine1 AlarmvalveAnandNessuna valutazione finora