Potrebbero piacerti anche
- Tshiluba Language Structures PDFDocumento3 pagineTshiluba Language Structures PDFFrancisco José Da SilvaNessuna valutazione finora
- Angiodroid Co2 InjectorDocumento55 pagineAngiodroid Co2 InjectorArnaud TORNIERNessuna valutazione finora
- Economic Analysis For RoboticsDocumento11 pagineEconomic Analysis For RoboticsMICHEL RAJ0% (1)
- Medical Imaging Field Service EngineerDocumento3 pagineMedical Imaging Field Service Engineerapi-78699586Nessuna valutazione finora
- Agricultural Mechanisation in Ghana - ReviewDocumento10 pagineAgricultural Mechanisation in Ghana - ReviewShadrack Kwadwo AmponsahNessuna valutazione finora
- Study of Maximum Power Point Tracking (MPPT) in PV SystemsDocumento10 pagineStudy of Maximum Power Point Tracking (MPPT) in PV SystemsabdalbarNessuna valutazione finora
- GZ Ia2p16 PDFDocumento1.200 pagineGZ Ia2p16 PDFTalha Riaz100% (1)
- Oxygen Concentrator 7F-5A User's Manual: Do Not Operate This Unit Without First Reading and Understanding This ManualDocumento13 pagineOxygen Concentrator 7F-5A User's Manual: Do Not Operate This Unit Without First Reading and Understanding This Manualkoko zaza100% (1)
- Real-World Micro Grids - An OverviewDocumento8 pagineReal-World Micro Grids - An Overviewkhanh_ngaNessuna valutazione finora
- Flattening Filter FreeDocumento2 pagineFlattening Filter Freeapi-337168367Nessuna valutazione finora
- Digital Marketing 1Documento385 pagineDigital Marketing 1evanaNessuna valutazione finora
- Bio-Medical Engineer CVDocumento4 pagineBio-Medical Engineer CVAkram SayeedNessuna valutazione finora
- GreenFlux Smart Charging Whitepaper LRDocumento19 pagineGreenFlux Smart Charging Whitepaper LRgstarmstar8490Nessuna valutazione finora
- Job Responsibility Checklist - RadiogrpherDocumento2 pagineJob Responsibility Checklist - Radiogrphertafi66Nessuna valutazione finora
- Customer Invoice Booking Ota Commission MGR54791 2021 10-31-030047597Documento2 pagineCustomer Invoice Booking Ota Commission MGR54791 2021 10-31-030047597Ravi ZombadeNessuna valutazione finora
- Cios Spin - BrochureDocumento36 pagineCios Spin - BrochureMauroNessuna valutazione finora
- DC30-091 DRX-Ascend System Operator Manual - MDocumento66 pagineDC30-091 DRX-Ascend System Operator Manual - MRaquel BedoyaNessuna valutazione finora
- Technical Training and Equipment: Review That Poor Broadband Connections Could Lead To "Possible Patient Mismanagement."Documento3 pagineTechnical Training and Equipment: Review That Poor Broadband Connections Could Lead To "Possible Patient Mismanagement."Melati CahyaniNessuna valutazione finora
- OT Design PDFDocumento12 pagineOT Design PDFKhalid KhassawnehNessuna valutazione finora
- Design Construction of One Uninterruptible Power Supply (UPS)Documento25 pagineDesign Construction of One Uninterruptible Power Supply (UPS)Suva nilNessuna valutazione finora
- Green Hospitals PDFDocumento56 pagineGreen Hospitals PDFJJ MMNessuna valutazione finora
- Bio Medical Engg FaqDocumento24 pagineBio Medical Engg FaqManojNessuna valutazione finora
- 1SDC007109G0203 QT10 Photovoltaic PlantsDocumento126 pagine1SDC007109G0203 QT10 Photovoltaic PlantsRandolf Wenhold100% (1)
- SanofiDocumento19 pagineSanofiAnsariRizzNessuna valutazione finora
- Adaptation and Use of Telemedicine in Saudi ArabiaDocumento4 pagineAdaptation and Use of Telemedicine in Saudi ArabiaGreat SingerNessuna valutazione finora
- Jamia Millia Islamia: Hospital Management SystemDocumento27 pagineJamia Millia Islamia: Hospital Management SystemzainjNessuna valutazione finora
- User Manual X RayDocumento130 pagineUser Manual X RayM Agung FatahillahNessuna valutazione finora
- Asset ManagementDocumento4 pagineAsset ManagementJohan TadlasNessuna valutazione finora
- IoT Based Industrial Information GatheringDocumento7 pagineIoT Based Industrial Information GatheringEditor IJTSRDNessuna valutazione finora
- SWOT Analysis of Pharmaceutical Industry Bangladesh HKH Ygg Iyhuih Iyhuihuih UyuhykhjDocumento2 pagineSWOT Analysis of Pharmaceutical Industry Bangladesh HKH Ygg Iyhuih Iyhuihuih UyuhykhjmyhellonearthNessuna valutazione finora
- The Role of Magnesium Sulfate MgSO4 in Fetal Neuroprotection PDFDocumento14 pagineThe Role of Magnesium Sulfate MgSO4 in Fetal Neuroprotection PDFniluh suwasantiNessuna valutazione finora
- IT Acts in India 2000Documento14 pagineIT Acts in India 2000KanchanNessuna valutazione finora
- Detail Project ReportDocumento149 pagineDetail Project ReportLal PeirisNessuna valutazione finora
- Mis of HospitalDocumento20 pagineMis of HospitalBindu PathakNessuna valutazione finora
- 34 - Design of Energy Monitoring System Based On IOTDocumento4 pagine34 - Design of Energy Monitoring System Based On IOTFelipe Osmar de AvizNessuna valutazione finora
- Solar DocsDocumento268 pagineSolar DocsSumit MishraNessuna valutazione finora
- Chapter 4 - Business Models: Learning ObjectivesDocumento7 pagineChapter 4 - Business Models: Learning ObjectivesMuhammad FaizanNessuna valutazione finora
- Vdocuments - MX Part II Cyclotrons For Radioisotope ProductionDocumento54 pagineVdocuments - MX Part II Cyclotrons For Radioisotope Productioncarolina100% (1)
- Gopal Gupta 2K20PES09-1Documento18 pagineGopal Gupta 2K20PES09-1Kritu Gupta100% (1)
- CT Buyers Guide 2-13Documento21 pagineCT Buyers Guide 2-13Mahmoud Ahmed50% (2)
- A Comprehensive Project Report ON "Feasibility Study of Solar Cell "Documento18 pagineA Comprehensive Project Report ON "Feasibility Study of Solar Cell "Chaitanya VaidyaNessuna valutazione finora
- Address: - Puranadhar Power Vision, PuneDocumento7 pagineAddress: - Puranadhar Power Vision, PuneDhanesh GaikwadNessuna valutazione finora
- ZENNER MNK Domestic Water-MetersDocumento48 pagineZENNER MNK Domestic Water-MetersEtc EtcNessuna valutazione finora
- Suragi Solar PlantDocumento33 pagineSuragi Solar Plantrangaswamy bnNessuna valutazione finora
- Glossary Health TeccnologyDocumento4 pagineGlossary Health TeccnologyreneportilloNessuna valutazione finora
- GSM (Global System For Mobile Communications) : Prepared by Muhammad ArifDocumento64 pagineGSM (Global System For Mobile Communications) : Prepared by Muhammad ArifmdssuetNessuna valutazione finora
- Solar Grid CodeDocumento5 pagineSolar Grid CodenooralhudNessuna valutazione finora
- QpEE2401 Power System Operation ControlDocumento22 pagineQpEE2401 Power System Operation ControlPrakash Chandran CNessuna valutazione finora
- Internship Report 1Documento27 pagineInternship Report 1Saarthak AgarwalNessuna valutazione finora
- Energy ConservationDocumento15 pagineEnergy ConservationManpreet KaurNessuna valutazione finora
- 2019 Price List: Inspector (CAWI, CWI, SCWI) Certified Welding Educator (CWE)Documento1 pagina2019 Price List: Inspector (CAWI, CWI, SCWI) Certified Welding Educator (CWE)SpancerNessuna valutazione finora
- Equipment MaintenanceDocumento12 pagineEquipment MaintenanceGabriel OgbuNessuna valutazione finora
- Team PowerBank WP8000 EDM enDocumento4 pagineTeam PowerBank WP8000 EDM enSofiane ChenNessuna valutazione finora
- Resident Physics Lectures: Radiography GeometryDocumento36 pagineResident Physics Lectures: Radiography GeometryLajja Parikh PatelNessuna valutazione finora
- IEEE STD 1547Documento4 pagineIEEE STD 1547elchicogrisNessuna valutazione finora
- Annexure-I List of Medical Equipments PDFDocumento12 pagineAnnexure-I List of Medical Equipments PDFHassan100% (1)
- Understanding Patient Flow in Hospitals Web FinalDocumento38 pagineUnderstanding Patient Flow in Hospitals Web Finalo.bafqeer1Nessuna valutazione finora
- Wearable Biosensor ReportDocumento21 pagineWearable Biosensor ReportVaibhav Jain100% (1)
- Seminar ReportDocumento22 pagineSeminar ReportArchana BrahmaNessuna valutazione finora
- Recent Advances in Mammography: DR - Suhas B Resident (MD Radio-DiagnosisDocumento69 pagineRecent Advances in Mammography: DR - Suhas B Resident (MD Radio-DiagnosisMassimo RiserboNessuna valutazione finora
- 29.5.23 Lab QuestionsDocumento6 pagine29.5.23 Lab Questionsvidi87Nessuna valutazione finora
- Weight Loss ChartDocumento1 paginaWeight Loss Chartvidi87Nessuna valutazione finora
- Tnea 2019 OverallDocumento94 pagineTnea 2019 Overallvidi87Nessuna valutazione finora
- An Introduction To Networking TerminologyDocumento18 pagineAn Introduction To Networking Terminologyvidi87Nessuna valutazione finora
- Automatic Identification and Elimination of Pectoral Muscle in Digital MammogramsDocumento4 pagineAutomatic Identification and Elimination of Pectoral Muscle in Digital Mammogramsvidi87Nessuna valutazione finora
- Graphics and Multimedia: Unit 1 2D PrimitivesDocumento36 pagineGraphics and Multimedia: Unit 1 2D Primitivesvidi87Nessuna valutazione finora
- CP7101 Design and Management of Computer Networks Important and Model Question PaperDocumento1 paginaCP7101 Design and Management of Computer Networks Important and Model Question PaperJai SharmaNessuna valutazione finora
- Rating Learning Object Quality With Distributed Bayesian Belief Networks: The Why and The HowDocumento3 pagineRating Learning Object Quality With Distributed Bayesian Belief Networks: The Why and The Howvidi87Nessuna valutazione finora
- Arasu Engineering College, Kumbakonam - 612 501: Department of ChemistryDocumento1 paginaArasu Engineering College, Kumbakonam - 612 501: Department of Chemistryvidi87Nessuna valutazione finora
- A Relatedness-Based Data-Driven Approach To Determination of Interestingness of Association RulesDocumento2 pagineA Relatedness-Based Data-Driven Approach To Determination of Interestingness of Association Rulesvidi87Nessuna valutazione finora
- On Optimal Rule Discovery: Jiuyong LiDocumento12 pagineOn Optimal Rule Discovery: Jiuyong Lividi87Nessuna valutazione finora
- Principles, Methods and Applications: Mike Uschold & Michael Gruninger AIAI-TR-191 February 1996Documento69 paginePrinciples, Methods and Applications: Mike Uschold & Michael Gruninger AIAI-TR-191 February 1996vidi87Nessuna valutazione finora
- Generating Non-Redundant Association RulesDocumento18 pagineGenerating Non-Redundant Association Rulesvidi87Nessuna valutazione finora
- Std10 Science EM 1Documento156 pagineStd10 Science EM 1vidi87Nessuna valutazione finora
- Gray To ColorDocumento6 pagineGray To Colorvidi87Nessuna valutazione finora
- OS Question BankDocumento24 pagineOS Question Bankvidi87Nessuna valutazione finora
- White Paper Cloud Computing ( (PDF, 351 KB) )Documento25 pagineWhite Paper Cloud Computing ( (PDF, 351 KB) )vidi87Nessuna valutazione finora
- U1 Escorting A Patient For TestsDocumento2 pagineU1 Escorting A Patient For TestsKlára BraunNessuna valutazione finora
- Evaluare Pacient - Scor HAS-BLED: H A S B L E DDocumento2 pagineEvaluare Pacient - Scor HAS-BLED: H A S B L E Dviorel79Nessuna valutazione finora
- Diagnostic CentreDocumento14 pagineDiagnostic CentreJonas AsiaNessuna valutazione finora
- Rsup. Dr. Wahidin Sudirohusodo Laporan OperasiDocumento2 pagineRsup. Dr. Wahidin Sudirohusodo Laporan OperasiRizkyastari OnnyNessuna valutazione finora
- Haemoglobin Percentage: Visit Id: R7758972Documento2 pagineHaemoglobin Percentage: Visit Id: R7758972iyengaarNessuna valutazione finora
- Inventaris IGD 2022 TerbaruDocumento5 pagineInventaris IGD 2022 TerbaruEryNessuna valutazione finora
- Charts CompiledDocumento6 pagineCharts CompiledMei Marie MangubatNessuna valutazione finora
- ResumefeliciachuDocumento2 pagineResumefeliciachuapi-450475136Nessuna valutazione finora
- LABORATORYDocumento6 pagineLABORATORYNikz BersalesNessuna valutazione finora
- Novalis TX RadiosurgeryDocumento0 pagineNovalis TX RadiosurgeryDenis MarcoNessuna valutazione finora
- Computed Radiography (CR) : Dosen: Anak Agung Aris Diartama, S.ST, M.TR - IDDocumento28 pagineComputed Radiography (CR) : Dosen: Anak Agung Aris Diartama, S.ST, M.TR - IDKevin TagahNessuna valutazione finora
- Helicobacter Pylori Stool Antigen TestDocumento4 pagineHelicobacter Pylori Stool Antigen TestAsri RachmawatiNessuna valutazione finora
- Breast Cancer Diagnostic Imaging in Dharmais Cancer HospitalDocumento32 pagineBreast Cancer Diagnostic Imaging in Dharmais Cancer HospitalIndonesian Journal of CancerNessuna valutazione finora
- Radiology and Imaging Equipment - Hospital Medical Imaging Equipment - MedpickDocumento30 pagineRadiology and Imaging Equipment - Hospital Medical Imaging Equipment - MedpickMedpickNessuna valutazione finora
- Week 1 IntroductionDocumento13 pagineWeek 1 Introductionobai AlhwimelNessuna valutazione finora
- Accesories Advanced Endoscopy Olympus PDFDocumento1 paginaAccesories Advanced Endoscopy Olympus PDFJawia YusranNessuna valutazione finora
- PUDV3134Documento1 paginaPUDV3134rakesh adamalaNessuna valutazione finora
- Resume MedisDocumento6 pagineResume MedisRina ekaNessuna valutazione finora
- Medical Equipments Catalogue RRV GlobalDocumento12 pagineMedical Equipments Catalogue RRV GlobalzeeshanNessuna valutazione finora
- AERB Guidelines RadiologyDocumento4 pagineAERB Guidelines RadiologyTejinder100% (1)
- Current Diagnostic Techniques in Veterinary Surgery PDFDocumento2 pagineCurrent Diagnostic Techniques in Veterinary Surgery PDFKirti JamwalNessuna valutazione finora
- Clear. Compact. Comprehensive: TransducersDocumento2 pagineClear. Compact. Comprehensive: TransducersAnny SriNessuna valutazione finora
- DR Diwan Chand AggarwalDocumento2 pagineDR Diwan Chand AggarwalMohit AggarwalNessuna valutazione finora
- National Cancer Institute 268/1 Rama 6 Road Thung Phaya Thai, Ratchathewi, Bangkok 10400 Tel. 02-202-6800, 02-202-6888Documento2 pagineNational Cancer Institute 268/1 Rama 6 Road Thung Phaya Thai, Ratchathewi, Bangkok 10400 Tel. 02-202-6800, 02-202-6888Choo HokiertiNessuna valutazione finora
- Lightspeed VCT XT: Ge HealthcareDocumento4 pagineLightspeed VCT XT: Ge HealthcareВалерий КоваленкоNessuna valutazione finora
- Breast Cancer Screening ResDocumento7 pagineBreast Cancer Screening Resomegasauron0gmailcomNessuna valutazione finora
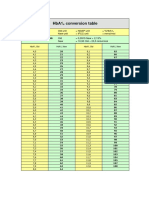
- HbA1cConversionTable PDFDocumento1 paginaHbA1cConversionTable PDFDarkoMaxNessuna valutazione finora
- Enterprise Imaging 8.0.x DICOM Conformance StatementDocumento124 pagineEnterprise Imaging 8.0.x DICOM Conformance Statementأحمد قائدNessuna valutazione finora
- Zoheir Aissaoui Rals03-10016Documento1 paginaZoheir Aissaoui Rals03-10016babelfirdaousNessuna valutazione finora
- Outscraper-2023110612255569c3 Pathology +1Documento590 pagineOutscraper-2023110612255569c3 Pathology +1OFC accountNessuna valutazione finora