Potrebbero piacerti anche
- JC 14Documento35 pagineJC 14BharathSimhaReddyDalliNessuna valutazione finora
- Avoiding and Treating Dental Complications: Best Practices in DentistryDa EverandAvoiding and Treating Dental Complications: Best Practices in DentistryDeborah A. TermeieNessuna valutazione finora
- Non-Surgical Treatment of Periapical Lesion Using Calcium Hydroxide-A Case ReportDocumento4 pagineNon-Surgical Treatment of Periapical Lesion Using Calcium Hydroxide-A Case ReportNadya PurwantyNessuna valutazione finora
- CBCT Article SandyDocumento9 pagineCBCT Article Sandysandeep lachhwaniNessuna valutazione finora
- Success& Failures in EndoDocumento32 pagineSuccess& Failures in Endorasagna reddyNessuna valutazione finora
- Healthcare 07 00120Documento9 pagineHealthcare 07 00120Ryantino IrdanNessuna valutazione finora
- A Prospective Evaluation of Factors Affecting Occ - 2020 - American Journal of ODocumento7 pagineA Prospective Evaluation of Factors Affecting Occ - 2020 - American Journal of OAlejandro Aranzábal NavarreteNessuna valutazione finora
- PalateDocumento41 paginePalatearif sudiantoNessuna valutazione finora
- Delyana Fitria Dewi 04031181320027Documento4 pagineDelyana Fitria Dewi 04031181320027Delyana Fitria DewiNessuna valutazione finora
- Radiologia en EndodonciaDocumento12 pagineRadiologia en EndodonciaBelez Jum JumNessuna valutazione finora
- Eickholz 1997Documento9 pagineEickholz 1997NareshNessuna valutazione finora
- Case SeriesDocumento7 pagineCase SerieskarthikNessuna valutazione finora
- LD Final PriyankaDocumento108 pagineLD Final PriyankaPriyanka GandhiNessuna valutazione finora
- Palatally Impacted Canines A NewDocumento9 paginePalatally Impacted Canines A Newplayer osamaNessuna valutazione finora
- Australian Dental Journal - 2009 - Corbet - Radiographs in Periodontal Disease Diagnosis and ManagementDocumento17 pagineAustralian Dental Journal - 2009 - Corbet - Radiographs in Periodontal Disease Diagnosis and Managementchloeyxy20001211Nessuna valutazione finora
- Kalwarf 1988 - Evaluation of Furcation Response To Perio TherapyDocumento11 pagineKalwarf 1988 - Evaluation of Furcation Response To Perio TherapyBryan HeeNessuna valutazione finora
- Recurrent Peripheral Odontogenic Keratocyst: A Case ReportDocumento3 pagineRecurrent Peripheral Odontogenic Keratocyst: A Case ReportthedocperuNessuna valutazione finora
- Digital Imaging in Trauma Part 2Documento9 pagineDigital Imaging in Trauma Part 2Gaurav BasuNessuna valutazione finora
- Effect of Gap Length and Position On Results of Treatment of Cancer of The Larynx in Scotland by Radiotherapy.. A Linear Quadratic AnalysisDocumento9 pagineEffect of Gap Length and Position On Results of Treatment of Cancer of The Larynx in Scotland by Radiotherapy.. A Linear Quadratic AnalysisrgergerNessuna valutazione finora
- Artikkel 2 OtfDocumento13 pagineArtikkel 2 OtfAyu Ervita HydayatyNessuna valutazione finora
- Root Resorption Diagnosed With Cone Beam Computed Tomography After 6 Months of Orthodontic Treatment With Fixed Appliance and The Relation To Risk FactorsDocumento6 pagineRoot Resorption Diagnosed With Cone Beam Computed Tomography After 6 Months of Orthodontic Treatment With Fixed Appliance and The Relation To Risk FactorsElla GolikNessuna valutazione finora
- 8 - Clinical Outcome in Periradicular Surgery Effect of Patient - and Tooth-Related Factors - A Multicenter StudyDocumento8 pagine8 - Clinical Outcome in Periradicular Surgery Effect of Patient - and Tooth-Related Factors - A Multicenter StudykochikaghochiNessuna valutazione finora
- Journal of Endodontics 2013 Ball - Henrik - Skjerven - 11!06!2013Documento10 pagineJournal of Endodontics 2013 Ball - Henrik - Skjerven - 11!06!2013Marilyn GonzalesNessuna valutazione finora
- Fundamentals of Oral and Maxillofacial RadiologyDa EverandFundamentals of Oral and Maxillofacial RadiologyValutazione: 4 su 5 stelle4/5 (1)
- 11 - Radiographic Parameters Biological Significance and Clinical Use - Periodontology 2000 - 2005 - BR Gger PDFDocumento18 pagine11 - Radiographic Parameters Biological Significance and Clinical Use - Periodontology 2000 - 2005 - BR Gger PDFm.castillo11Nessuna valutazione finora
- Modified Technique of Radical Inguinal Lymphadenectomy For Penile Carcinoma: Morbidity and OutcomeDocumento7 pagineModified Technique of Radical Inguinal Lymphadenectomy For Penile Carcinoma: Morbidity and OutcomeAlwin PrasetyaNessuna valutazione finora
- Case Report Treatment of An Adult Skeletal Class III Patient With Surgically Assisted Rapid Palatal Expansion and FacemaskDocumento7 pagineCase Report Treatment of An Adult Skeletal Class III Patient With Surgically Assisted Rapid Palatal Expansion and FacemaskMirza GlusacNessuna valutazione finora
- Jurnal 2Documento4 pagineJurnal 2Eugunia EdgarNessuna valutazione finora
- Endodontic Topics Volume 19 Issue 1 2008 (Doi 10.1111/j.1601-1546.2011.00253.x) CHANKHRIT SATHORN PETER PARASHOS - Monitoring The Outcomes of Root Canal Re-TreatmentsDocumento10 pagineEndodontic Topics Volume 19 Issue 1 2008 (Doi 10.1111/j.1601-1546.2011.00253.x) CHANKHRIT SATHORN PETER PARASHOS - Monitoring The Outcomes of Root Canal Re-TreatmentsardeleanoanaNessuna valutazione finora
- Torabinejad 2018Documento6 pagineTorabinejad 2018viena mutmainnahNessuna valutazione finora
- ENDO Aae-Aaomr-2015updateDocumento7 pagineENDO Aae-Aaomr-2015updateSara MoustafaNessuna valutazione finora
- LEUKAEMIA AND ORTHDONTICS by AlmuzianDocumento3 pagineLEUKAEMIA AND ORTHDONTICS by AlmuzianRahulLife'sNessuna valutazione finora
- 2018 Torabinejad Periapical Radiolucencies Using CBCT JOEDocumento6 pagine2018 Torabinejad Periapical Radiolucencies Using CBCT JOEJonatan Arroyo BautistaNessuna valutazione finora
- Large Lesion Management - Roots0112Documento4 pagineLarge Lesion Management - Roots0112nuriacampoNessuna valutazione finora
- Case Report: Resolution of Localized Chronic Periodontitis Associated With Longstanding Calculus DepositsDocumento7 pagineCase Report: Resolution of Localized Chronic Periodontitis Associated With Longstanding Calculus DepositsAkbar SyadaNessuna valutazione finora
- Postretention Mandibular Incisor Stability After Premo - 1999 - Seminars in OrthDocumento10 paginePostretention Mandibular Incisor Stability After Premo - 1999 - Seminars in OrthNIKHITANessuna valutazione finora
- RetrieveDocumento7 pagineRetrieve01 X A.A. Gede Reynata Putra XII MIPA 4Nessuna valutazione finora
- Lasers: Effect of Low-Level Laser Therapy and Platelet-Rich Fibrin On The Treatment of Intra-Bony DefectsDocumento8 pagineLasers: Effect of Low-Level Laser Therapy and Platelet-Rich Fibrin On The Treatment of Intra-Bony DefectsMegha PoojaryNessuna valutazione finora
- Tic Treatment of Teeth With Apical Period On Tit Is Single vs. Multi Visit TreatmentDocumento6 pagineTic Treatment of Teeth With Apical Period On Tit Is Single vs. Multi Visit Treatmentgpv38Nessuna valutazione finora
- 2012 Effects of RT in Head and NeckDocumento10 pagine2012 Effects of RT in Head and NeckCamiDavidNessuna valutazione finora
- 2016 - Diagnostic Features and Management Strategy of A Refractory Case of Radionecrosis of The MandibleDocumento12 pagine2016 - Diagnostic Features and Management Strategy of A Refractory Case of Radionecrosis of The MandibleSyifa IKNessuna valutazione finora
- Radiotherapy of Liver CancerDa EverandRadiotherapy of Liver CancerJinsil SeongNessuna valutazione finora
- Treatment of A Large Maxillary Cyst With MarsupializationDocumento8 pagineTreatment of A Large Maxillary Cyst With MarsupializationDinesh SolankiNessuna valutazione finora
- FESS de RevisiónDocumento7 pagineFESS de RevisiónMarco Antonio FigueroaNessuna valutazione finora
- Minimally Invasive Periodontal Therapy: Clinical Techniques and Visualization TechnologyDa EverandMinimally Invasive Periodontal Therapy: Clinical Techniques and Visualization TechnologyNessuna valutazione finora
- Radiographic Aids in DX of Periodontol Ds - Part ADocumento53 pagineRadiographic Aids in DX of Periodontol Ds - Part ADrIbrahimShaikhNessuna valutazione finora
- 1 s2.0 S036030160503097X MainDocumento7 pagine1 s2.0 S036030160503097X MainLuis Felipe Varela EspinozaNessuna valutazione finora
- hpb0016 0001Documento2 paginehpb0016 0001Yacine Tarik AizelNessuna valutazione finora
- Nigro1991 (Si Desaparece Totalmente, No Biopsiar)Documento5 pagineNigro1991 (Si Desaparece Totalmente, No Biopsiar)ouf81Nessuna valutazione finora
- Radiology in PeriodonticsDocumento0 pagineRadiology in PeriodonticsMohamed Abd El-Fattah GalalNessuna valutazione finora
- Rectal CancerDocumento4 pagineRectal CancerAlice AugustinNessuna valutazione finora
- Periapical Bone Healing After ApicectomyDocumento5 paginePeriapical Bone Healing After ApicectomyMarwa Wagih ElboraeyNessuna valutazione finora
- M29918 v1 632975457331847500Documento8 pagineM29918 v1 632975457331847500Rizko WiraNessuna valutazione finora
- Background: Concurrent Chemoradiotherapy (CRT) Is The: Correspondence To: DR A.S.C. Wong, Department of HematologyDocumento11 pagineBackground: Concurrent Chemoradiotherapy (CRT) Is The: Correspondence To: DR A.S.C. Wong, Department of HematologyJordan SantosNessuna valutazione finora
- Management of A Large Radicular Cyst: A Non Surgical Endodontic ApproachDocumento4 pagineManagement of A Large Radicular Cyst: A Non Surgical Endodontic ApproachKranti PrajapatiNessuna valutazione finora
- Seehra2012 AJODO Retrospectivo MáscaraDocumento6 pagineSeehra2012 AJODO Retrospectivo MáscaraYeimi ArdilaNessuna valutazione finora
- Diff Betwn Inlay and Amalgam CavityDocumento7 pagineDiff Betwn Inlay and Amalgam CavityVinisha Vipin Sharma100% (1)
- Criteria of SelectionDocumento12 pagineCriteria of SelectionVinisha Vipin SharmaNessuna valutazione finora
- Acupuncture in Dentistry PDFDocumento73 pagineAcupuncture in Dentistry PDFVinisha Vipin SharmaNessuna valutazione finora
- Non Surgical Management of Periapical Lesions Using Calcium HydroxideDocumento6 pagineNon Surgical Management of Periapical Lesions Using Calcium HydroxideVinisha Vipin SharmaNessuna valutazione finora
- Mechanical Preparation Updated May2017 Prof Marco VersianiDocumento159 pagineMechanical Preparation Updated May2017 Prof Marco VersianiVinisha Vipin SharmaNessuna valutazione finora
- Challenges in Working Length DeterminationDocumento101 pagineChallenges in Working Length DeterminationVinisha Vipin SharmaNessuna valutazione finora
- Some Basics of LasersDocumento102 pagineSome Basics of LasersVinisha Vipin SharmaNessuna valutazione finora
- Laser in Conservative Dentistry & EndodonticsDocumento75 pagineLaser in Conservative Dentistry & EndodonticsVinisha Vipin SharmaNessuna valutazione finora
- Content ServerDocumento5 pagineContent ServerVinisha Vipin SharmaNessuna valutazione finora
- Show TextDocumento1 paginaShow TextVinisha Vipin SharmaNessuna valutazione finora
- Pin Retained RestorationDocumento31 paginePin Retained RestorationVinisha Vipin SharmaNessuna valutazione finora
- Eaat 14 I 1 P 217Documento6 pagineEaat 14 I 1 P 217Vinisha Vipin SharmaNessuna valutazione finora
- Glide Path PreparationDocumento5 pagineGlide Path PreparationVinisha Vipin SharmaNessuna valutazione finora
- EchsDocumento20 pagineEchsVinisha Vipin SharmaNessuna valutazione finora
- Content ServerDocumento6 pagineContent ServerVinisha Vipin SharmaNessuna valutazione finora
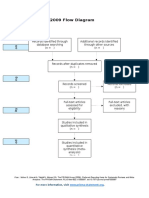
- PRISMA-P Statement - Moher Sys Rev Jan 2015Documento9 paginePRISMA-P Statement - Moher Sys Rev Jan 2015Vinisha Vipin SharmaNessuna valutazione finora
- PRISMA 2009 Flow Diagram: For More Information, VisitDocumento1 paginaPRISMA 2009 Flow Diagram: For More Information, VisitVinisha Vipin SharmaNessuna valutazione finora
- Dentin HypersensitivityDocumento62 pagineDentin HypersensitivityVinisha Vipin Sharma100% (1)
- Ceramic Restorations: Bonded Porcelain Veneers - Part 1: PerspectiveDocumento5 pagineCeramic Restorations: Bonded Porcelain Veneers - Part 1: PerspectiveVinisha Vipin SharmaNessuna valutazione finora
- Esthetic Alternatives To AmalgamDocumento15 pagineEsthetic Alternatives To AmalgamVinisha Vipin SharmaNessuna valutazione finora
- Clarks Cavity PreparationDocumento10 pagineClarks Cavity PreparationVinisha Vipin SharmaNessuna valutazione finora
- Nanodentistry: New Buzz in Dentistry: Review ArticleDocumento5 pagineNanodentistry: New Buzz in Dentistry: Review ArticleVinisha Vipin SharmaNessuna valutazione finora
- DaweDocumento41 pagineDawemichaelwillsonNessuna valutazione finora
- Copies of The Policy of The FollowingDocumento1 paginaCopies of The Policy of The FollowingPAULBENEDICT CATAQUIZNessuna valutazione finora
- Presentation1HAND WASHINGDocumento48 paginePresentation1HAND WASHINGDerick SemNessuna valutazione finora
- NUTRICION Y RENDIMIENTO DEPORTIVO Unlocked PDFDocumento40 pagineNUTRICION Y RENDIMIENTO DEPORTIVO Unlocked PDFRaúl Alejandro CubosNessuna valutazione finora
- MANUAL NeoRhythm 15122022Documento15 pagineMANUAL NeoRhythm 15122022Ch RehpotsirhcNessuna valutazione finora
- Health Care ReformsDocumento30 pagineHealth Care Reformssimonjosan75% (4)
- Chapter 1 Overview of Critical Care StudentDocumento40 pagineChapter 1 Overview of Critical Care StudentEmilyNessuna valutazione finora
- NY Abortion LawsDocumento1 paginaNY Abortion LawsManidhaNessuna valutazione finora
- MAKE YOUR PRACTICE FLOURISH WITH FERTILITY NUTRITION - Workbook PDFDocumento8 pagineMAKE YOUR PRACTICE FLOURISH WITH FERTILITY NUTRITION - Workbook PDFHershey AngelesNessuna valutazione finora
- B.D.S Third Year Examination Tabulation ChartDocumento22 pagineB.D.S Third Year Examination Tabulation ChartRoshan barikNessuna valutazione finora
- Bone Augmentation of The Edentulous Maxilla For Implant Placement: A Systematic ReviewDocumento12 pagineBone Augmentation of The Edentulous Maxilla For Implant Placement: A Systematic ReviewJarvin Miguel Buitrago GalindezNessuna valutazione finora
- Australia and Taiwan's Memorandum of Understanding - Medical TransfersDocumento12 pagineAustralia and Taiwan's Memorandum of Understanding - Medical TransfersBuzzFeedOz100% (1)
- Inst - Leg. Visa 482Documento27 pagineInst - Leg. Visa 482LucasNessuna valutazione finora
- Tackling HIV/AIDS and Malaria in PregnancyDocumento8 pagineTackling HIV/AIDS and Malaria in PregnancyCecilia McCallumNessuna valutazione finora
- Family Nursing Care Plan-ChnDocumento3 pagineFamily Nursing Care Plan-ChnChristine SaliganNessuna valutazione finora
- NCM110 NI CompiledNotesDocumento6 pagineNCM110 NI CompiledNotesSherinne Jane CariazoNessuna valutazione finora
- Penilaian Preceptorship (Mini-Cex, Dops, Longcase, Soca) 2020Documento49 paginePenilaian Preceptorship (Mini-Cex, Dops, Longcase, Soca) 2020Dian tri febrianaNessuna valutazione finora
- Trust Lap A Simulation Case StudyDocumento11 pagineTrust Lap A Simulation Case StudyApurv GautamNessuna valutazione finora
- Fast HugDocumento41 pagineFast HugBharti NaraNessuna valutazione finora
- Summative Evaluation Fall 2014 PortfolioDocumento3 pagineSummative Evaluation Fall 2014 Portfolioapi-312540648Nessuna valutazione finora
- Chapter 2Documento8 pagineChapter 2Es Claro100% (1)
- 325 - Unit 3.1Documento2 pagine325 - Unit 3.1IvanNessuna valutazione finora
- Veteran Help-Seeking Behaviour For Mental HealthDocumento6 pagineVeteran Help-Seeking Behaviour For Mental HealthDaniel KoffmanNessuna valutazione finora
- ATI Medication FormDocumento5 pagineATI Medication FormElaine De Vera100% (1)
- Curriculum Advanced Specialised Training Emergency MedicineDocumento35 pagineCurriculum Advanced Specialised Training Emergency MedicineSenthooran ArudshivsmNessuna valutazione finora
- Muguni Brandan ProposalDocumento31 pagineMuguni Brandan ProposalbonfaceNessuna valutazione finora
- Evidence Levels of Parafunctional Habits As Prominent Etiology in Facial Arthromyalgia: A Systematic ReviewDocumento7 pagineEvidence Levels of Parafunctional Habits As Prominent Etiology in Facial Arthromyalgia: A Systematic ReviewStacia AnastashaNessuna valutazione finora
- The Handbook of SalutogenesisDocumento634 pagineThe Handbook of SalutogenesisAna EclipseNessuna valutazione finora
- Fluoride Varnish ManualDocumento22 pagineFluoride Varnish ManualMaya SafitriNessuna valutazione finora
- Checklist For CritiqueDocumento2 pagineChecklist For CritiqueLiw RekoohNessuna valutazione finora