Potrebbero piacerti anche
- PH.D PROPOSAL BY N SRINU, UNIVERSITY OF HYDERABADDocumento9 paginePH.D PROPOSAL BY N SRINU, UNIVERSITY OF HYDERABADsri_cbmNessuna valutazione finora
- Litrature Review of Rural Healthcare Management in IndiaDocumento42 pagineLitrature Review of Rural Healthcare Management in Indiasri_cbm67% (6)
- PH.D PROPOSAL BY N SRINU, UNIVERSITY OF HYDERABADDocumento9 paginePH.D PROPOSAL BY N SRINU, UNIVERSITY OF HYDERABADsri_cbmNessuna valutazione finora
- Emergency Management Research Instutions in IndiaDocumento19 pagineEmergency Management Research Instutions in Indiasri_cbmNessuna valutazione finora
- Healthcare Financing Infrastructure PaperDocumento25 pagineHealthcare Financing Infrastructure Papersri_cbmNessuna valutazione finora
- Rural Healthcare Financing Management PaperDocumento21 pagineRural Healthcare Financing Management Papersri_cbmNessuna valutazione finora
- Primary Healthcare Management PaperDocumento18 paginePrimary Healthcare Management Papersri_cbmNessuna valutazione finora
- Iabe Paper 2010 ConferanceDocumento6 pagineIabe Paper 2010 Conferancesri_cbmNessuna valutazione finora
- Research Report Healthcare Delivery Management To Improve The Primary Healthcare Services and Universal Health Care in ThailandDocumento49 pagineResearch Report Healthcare Delivery Management To Improve The Primary Healthcare Services and Universal Health Care in Thailandsri_cbm0% (1)
- Research Report Healthcare Delivery Management To Improve The Primary Healthcare Services and Universal Health Care in ThailandDocumento49 pagineResearch Report Healthcare Delivery Management To Improve The Primary Healthcare Services and Universal Health Care in Thailandsri_cbm0% (1)
- I Am Sreenu. This My My Mahasarkham Research Report. I Cam From India For Resear Exchage Programm PurposeDocumento1 paginaI Am Sreenu. This My My Mahasarkham Research Report. I Cam From India For Resear Exchage Programm Purposesri_cbmNessuna valutazione finora
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (895)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (400)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (588)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (74)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (345)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2259)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (121)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- A Project Management Bench Mark: Delhi MetroDocumento26 pagineA Project Management Bench Mark: Delhi Metrodineshsoni29685Nessuna valutazione finora
- Kuis Pengauditan 1 Chapter 8,9,10Documento7 pagineKuis Pengauditan 1 Chapter 8,9,10Matus HanunNessuna valutazione finora
- Microsoft Financial Reporting Strategy SolutionDocumento3 pagineMicrosoft Financial Reporting Strategy Solutionmawiesya100% (1)
- Startup India Standup IndiaDocumento6 pagineStartup India Standup IndiaabhaybittuNessuna valutazione finora
- Walter Model Equity ValuationDocumento13 pagineWalter Model Equity ValuationVaidyanathan RavichandranNessuna valutazione finora
- Labuan Tax FrameworkDocumento8 pagineLabuan Tax FrameworkPhilippe PandyNessuna valutazione finora
- Types of RisksDocumento3 pagineTypes of RisksayushdixitNessuna valutazione finora
- Benefits of Aviation Brazil 2011 IATADocumento28 pagineBenefits of Aviation Brazil 2011 IATAKatia Mantovani MirandaNessuna valutazione finora
- Cadbury 2007 Annual Report & AccountsDocumento153 pagineCadbury 2007 Annual Report & AccountsChike Chukudebelu100% (1)
- ACCT 102 Lecture Notes Chapter 15 SPR 2016Documento4 pagineACCT 102 Lecture Notes Chapter 15 SPR 2016xenoyewNessuna valutazione finora
- Math MistakessssssDocumento3 pagineMath MistakessssssTravis GordonNessuna valutazione finora
- SFM Formulas Sheet For Quick Revision Before ExamDocumento28 pagineSFM Formulas Sheet For Quick Revision Before ExamKamakshi AdadadiNessuna valutazione finora
- Research Project PrintedDocumento49 pagineResearch Project PrintedNiharika ShahNessuna valutazione finora
- Analysis of Working Capital Management: A Project Report OnDocumento39 pagineAnalysis of Working Capital Management: A Project Report OngitarghawaleNessuna valutazione finora
- Module 9 Bustaxa InputvatDocumento16 pagineModule 9 Bustaxa Inputvatdennis delrosarioNessuna valutazione finora
- 2 BXooo 006610620000 R 969253 A0 FFC521Documento1 pagina2 BXooo 006610620000 R 969253 A0 FFC521Pily AguilarNessuna valutazione finora
- Bilans Uspeha - PROFIT AND LOSS ACCOUNTDocumento2 pagineBilans Uspeha - PROFIT AND LOSS ACCOUNTLorimer010100% (7)
- PPT For Corporate ActionsDocumento29 paginePPT For Corporate Actionshimanshu9899Nessuna valutazione finora
- Assignment - 2 Cash Flow Analysis: Submitted by Group - 8Documento13 pagineAssignment - 2 Cash Flow Analysis: Submitted by Group - 8dheeraj_rai005Nessuna valutazione finora
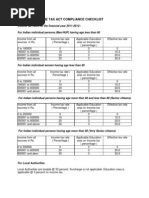
- 53.income Tax Compliance Check ListDocumento5 pagine53.income Tax Compliance Check ListmercatuzNessuna valutazione finora
- Business Plan: Acme Training Services & Computer SalesDocumento8 pagineBusiness Plan: Acme Training Services & Computer SalesMaria Rhakhen Regunda AnclaNessuna valutazione finora
- Media Nusantara Citra TBK.: Company Report: January 2019 As of 31 January 2019Documento3 pagineMedia Nusantara Citra TBK.: Company Report: January 2019 As of 31 January 2019Paras FebriayuniNessuna valutazione finora
- Beiersdorf Annual Report 2018Documento106 pagineBeiersdorf Annual Report 2018Ninad KhareNessuna valutazione finora
- Chapter 2 Accounting For Accruals and Deferrals: Fundamental Financial Accounting Concepts, 10e (Edmonds)Documento45 pagineChapter 2 Accounting For Accruals and Deferrals: Fundamental Financial Accounting Concepts, 10e (Edmonds)brockNessuna valutazione finora
- Source Booklet Jan 09 6001Documento12 pagineSource Booklet Jan 09 6001MashiatUddinNessuna valutazione finora
- The Greek Debt CrisisDocumento14 pagineThe Greek Debt CrisisTimothy Tan100% (2)
- Ind As 8 PDFDocumento56 pagineInd As 8 PDFmanan3466Nessuna valutazione finora
- Hilton 13e SM Ch07Documento72 pagineHilton 13e SM Ch07tttNessuna valutazione finora
- Rules of Capital Maintenance: Pranjal NeupaneDocumento11 pagineRules of Capital Maintenance: Pranjal NeupaneSamish DhakalNessuna valutazione finora
- The Trader Business PlanDocumento4 pagineThe Trader Business Planmitesh100% (4)