Potrebbero piacerti anche
- Stevens' Handbook of Experimental Psychology and Cognitive Neuroscience, Sensation, Perception, and AttentionDa EverandStevens' Handbook of Experimental Psychology and Cognitive Neuroscience, Sensation, Perception, and AttentionNessuna valutazione finora
- Poster VanhoomissenDocumento1 paginaPoster VanhoomissenBachelorproef TPNessuna valutazione finora
- The Statistical Analysis of Quasi-ExperimentsDa EverandThe Statistical Analysis of Quasi-ExperimentsNessuna valutazione finora
- Visual Acuity VarianceDocumento8 pagineVisual Acuity VarianceizzuddinhairolNessuna valutazione finora
- Ignal Etection Heory: Instructors: J.L. Szalma and P.A. HancockDocumento6 pagineIgnal Etection Heory: Instructors: J.L. Szalma and P.A. HancockLeonardoNessuna valutazione finora
- An Analysis-Of-Variance Model For The Assessment of Configural Cue Utilization in Clinical JudgmentDocumento12 pagineAn Analysis-Of-Variance Model For The Assessment of Configural Cue Utilization in Clinical JudgmentaitorNessuna valutazione finora
- Rational Theory of Cognition in PsychologyDocumento5 pagineRational Theory of Cognition in PsychologyPetrovic UrosNessuna valutazione finora
- 2013 Kendrick KayDocumento15 pagine2013 Kendrick KayDr-Raheel ZafarNessuna valutazione finora
- Artigo Stevens 1971Documento25 pagineArtigo Stevens 1971Rodrigo Ramón Falconi GómezNessuna valutazione finora
- Neural Networks: Arlex Oscar Marín García, Markus Franziskus Müller, Kaspar Schindler, Christian RummelDocumento11 pagineNeural Networks: Arlex Oscar Marín García, Markus Franziskus Müller, Kaspar Schindler, Christian RummelAki SunshinNessuna valutazione finora
- Personality traits and lucid dreaming frequencyDocumento11 paginePersonality traits and lucid dreaming frequencyMarina AlexopoulouNessuna valutazione finora
- Lucid DreamingDocumento11 pagineLucid DreamingMarina AlexopoulouNessuna valutazione finora
- Test t distribution introductionDocumento5 pagineTest t distribution introductionthishaniNessuna valutazione finora
- Subjects? Reliability: Consistency or Differentiating Among: Phys TherDocumento4 pagineSubjects? Reliability: Consistency or Differentiating Among: Phys TherMostafa AbdelrahmanNessuna valutazione finora
- PhysicsloveDocumento6 paginePhysicsloveJean Tañala BagueNessuna valutazione finora
- KappaDocumento2 pagineKappaJose Jose HuaNessuna valutazione finora
- Rcihards 1993 Spurius CorrelationDocumento14 pagineRcihards 1993 Spurius CorrelationFlorencia StelzerNessuna valutazione finora
- IMP IMP LinschotenDocumento18 pagineIMP IMP LinschotenSanjay LungareNessuna valutazione finora
- At What Sample Size Do Correlations StabilizeDocumento12 pagineAt What Sample Size Do Correlations Stabilizeanjana2014Nessuna valutazione finora
- Analysis of Facial Skin Thickness: Defining The Relative Thickness IndexDocumento5 pagineAnalysis of Facial Skin Thickness: Defining The Relative Thickness Indexxj112358Nessuna valutazione finora
- TPC Paper AllisonwrightDocumento9 pagineTPC Paper Allisonwrightapi-632741700Nessuna valutazione finora
- Contrast Sensitivity Measured by Two Methods in Young AdultsDocumento8 pagineContrast Sensitivity Measured by Two Methods in Young AdultsCEBNessuna valutazione finora
- The Mastoid Air-Cell SystemDocumento34 pagineThe Mastoid Air-Cell SystemAthiyatunAnnisaNessuna valutazione finora
- PEFR measured with Wright peak flow metersDocumento4 paginePEFR measured with Wright peak flow metersEthan XuNessuna valutazione finora
- Agewise Variation of Intraocular Pressure, Pachymetryand Keratometry in The Urban Areas of AssamDocumento4 pagineAgewise Variation of Intraocular Pressure, Pachymetryand Keratometry in The Urban Areas of AssamInternational Organization of Scientific Research (IOSR)Nessuna valutazione finora
- The Irregularity Index, A Quantitative Score of Mandibular Anterior Alignment-LittleDocumento10 pagineThe Irregularity Index, A Quantitative Score of Mandibular Anterior Alignment-LittlepveginaduNessuna valutazione finora
- On Mantel HaenszelDocumento3 pagineOn Mantel HaenszelAnonymous rfn4FLKD8Nessuna valutazione finora
- Sample SizeDocumento13 pagineSample SizeMuhammad RiyadhNessuna valutazione finora
- Hint Z Man Caul Ton Curran 94Documento15 pagineHint Z Man Caul Ton Curran 94Denisa BalajNessuna valutazione finora
- My Educational FieldDocumento27 pagineMy Educational FieldMaria KanwalNessuna valutazione finora
- 1 s2.0 S0042698917300937 Main 2Documento11 pagine1 s2.0 S0042698917300937 Main 2aprivatesyaNessuna valutazione finora
- Ashwin Visualacuityautism bp08 PDFDocumento5 pagineAshwin Visualacuityautism bp08 PDFrkNessuna valutazione finora
- Go L Diamond 1958Documento39 pagineGo L Diamond 1958Delia BucurNessuna valutazione finora
- C Rider 1993Documento14 pagineC Rider 1993Magda MoldovanNessuna valutazione finora
- Reply To: No Specific Relationship Between Hypnotic Suggestibility and The Rubber Hand IllusionDocumento4 pagineReply To: No Specific Relationship Between Hypnotic Suggestibility and The Rubber Hand IllusionKamoKamoNessuna valutazione finora
- Research JustificationDocumento6 pagineResearch JustificationGeorge DennisonNessuna valutazione finora
- Methods For Normalization of Hippocampal VolumesDocumento7 pagineMethods For Normalization of Hippocampal VolumesmarkecbNessuna valutazione finora
- Øving BA 2Documento12 pagineØving BA 2Erik CarlströmNessuna valutazione finora
- RSA5 JournalDocumento20 pagineRSA5 JournalDimitris GrigoriouNessuna valutazione finora
- NH Màn Hình 2023-02-10 Lúc 14.11.27Documento3 pagineNH Màn Hình 2023-02-10 Lúc 14.11.27hoàng nguyễnNessuna valutazione finora
- Statistical Treatment of Data, Data Interpretation, and ReliabilityDocumento6 pagineStatistical Treatment of Data, Data Interpretation, and Reliabilitydraindrop8606Nessuna valutazione finora
- Visual Analog ScalesDocumento6 pagineVisual Analog ScaleshsnhsynNessuna valutazione finora
- Approaching Myopia Holistic AllyDocumento7 pagineApproaching Myopia Holistic AllysoloiosochisonoNessuna valutazione finora
- Consistency of Ao Fracture Classification For The Distal RadiusDocumento6 pagineConsistency of Ao Fracture Classification For The Distal RadiusNatalie AlvaradoNessuna valutazione finora
- Michelson Contrast Sensitivity PDFDocumento5 pagineMichelson Contrast Sensitivity PDFPradit SaraonNessuna valutazione finora
- Is Postural Platform Suited To Study Correlations Between The Masticatory System and Body PostureDocumento8 pagineIs Postural Platform Suited To Study Correlations Between The Masticatory System and Body PostureAndreaVanoyMartinNessuna valutazione finora
- Kilby 2012Documento4 pagineKilby 2012DOUTOR HérniaNessuna valutazione finora
- Anatomy and Physiology of the Eye ReportDocumento12 pagineAnatomy and Physiology of the Eye ReportNashNessuna valutazione finora
- Morris 2Documento22 pagineMorris 2IsmaelLouGomezNessuna valutazione finora
- Carpal Tunnel Syndrome - The Role of Occupational FactorsDocumento12 pagineCarpal Tunnel Syndrome - The Role of Occupational Factorsgkmdmrh8m9Nessuna valutazione finora
- The Correlation Between Migraine Headache And.10Documento6 pagineThe Correlation Between Migraine Headache And.10Luther ThengNessuna valutazione finora
- Measures of Effect SizeDocumento11 pagineMeasures of Effect SizeXiang-Yang LouNessuna valutazione finora
- TH0311-1/90/0000/0337/$01.00 1990 IEEE: Dia :nosticDocumento9 pagineTH0311-1/90/0000/0337/$01.00 1990 IEEE: Dia :nosticLaura Aguiar MartinhoNessuna valutazione finora
- ClaheDocumento9 pagineClaheLaura Aguiar MartinhoNessuna valutazione finora
- Estimators Due To A Finite Number of Spikes Correcting The Bias of Spike Field CoherenceDocumento12 pagineEstimators Due To A Finite Number of Spikes Correcting The Bias of Spike Field CoherenceelibathNessuna valutazione finora
- Concordance C Index - 2 PDFDocumento8 pagineConcordance C Index - 2 PDFnuriyesanNessuna valutazione finora
- Pelli 1988 ChartDocumento12 paginePelli 1988 ChartSunny KhaliqNessuna valutazione finora
- 1991 Metcalfe 1991 Recognition Failure and The Composite Memory Trace in CHARMDocumento25 pagine1991 Metcalfe 1991 Recognition Failure and The Composite Memory Trace in CHARMhoorieNessuna valutazione finora
- Kunst-Wilson (1980) Affective Discrimination of Stimuli That Cannot Be RecognizedDocumento2 pagineKunst-Wilson (1980) Affective Discrimination of Stimuli That Cannot Be RecognizedJohn TownsendNessuna valutazione finora
- ContinuousDocumento11 pagineContinuousDinaol TikuNessuna valutazione finora
- Anaesthesia Questions: Dr. Farzan Syed, Dr. Jai Prakash GuptaDocumento72 pagineAnaesthesia Questions: Dr. Farzan Syed, Dr. Jai Prakash Guptaarchana100% (1)
- PSY402C09Documento46 paginePSY402C09archanaNessuna valutazione finora
- Turkistan IDocumento2 pagineTurkistan IarchanaNessuna valutazione finora
- Pre-Op Assessment GuidelineDocumento45 paginePre-Op Assessment GuidelinearchanaNessuna valutazione finora
- Identifying and Assessing Anxiety in Pre-Operative PatientsDocumento1 paginaIdentifying and Assessing Anxiety in Pre-Operative PatientsarchanaNessuna valutazione finora
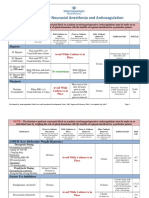
- Guidelines For Neuraxial Anesthesia and Anticoagulation: HeparinDocumento4 pagineGuidelines For Neuraxial Anesthesia and Anticoagulation: HeparinarchanaNessuna valutazione finora
- Pre-Op Assessment GuidelineDocumento45 paginePre-Op Assessment GuidelinearchanaNessuna valutazione finora
- NiceDocumento2 pagineNicearchanaNessuna valutazione finora
- ASA GuidelinesDocumento34 pagineASA GuidelinesarchanaNessuna valutazione finora
- Efficacy and Safety of Melatonin As An Anxiolytic and Analgesic in The Perioperative PeriodDocumento9 pagineEfficacy and Safety of Melatonin As An Anxiolytic and Analgesic in The Perioperative PeriodarchanaNessuna valutazione finora
- Zeev K NDocumento6 pagineZeev K NarchanaNessuna valutazione finora
- Jan LDeDocumento6 pagineJan LDearchanaNessuna valutazione finora
- Melatonin vs. Midazolam Premedication in Children: A Double-Blind, Placebo-Controlled StudyDocumento2 pagineMelatonin vs. Midazolam Premedication in Children: A Double-Blind, Placebo-Controlled StudyarchanaNessuna valutazione finora
- J R WittenbornDocumento7 pagineJ R WittenbornarchanaNessuna valutazione finora
- Naguib 2000Documento7 pagineNaguib 2000archanaNessuna valutazione finora
- Effect of Benzodiazepine Hypnotics On All-Night Sleep EEG SpectraDocumento1 paginaEffect of Benzodiazepine Hypnotics On All-Night Sleep EEG SpectraarchanaNessuna valutazione finora
- Premedication With Melatonin: A Double-Blind, Placebo-Controlled Comparison With MidazolamDocumento4 paginePremedication With Melatonin: A Double-Blind, Placebo-Controlled Comparison With MidazolamarchanaNessuna valutazione finora
- Naguib 2006Documento5 pagineNaguib 2006archanaNessuna valutazione finora
- Effect of Benzodiazepine Hypnotics On All-Night Sleep EEG SpectraDocumento1 paginaEffect of Benzodiazepine Hypnotics On All-Night Sleep EEG SpectraarchanaNessuna valutazione finora
- M CapuzzoDocumento3 pagineM CapuzzoarchanaNessuna valutazione finora
- Appendix 3. Pre-Operative Haemoglobin Optimisation For Elective SurgeryDocumento2 pagineAppendix 3. Pre-Operative Haemoglobin Optimisation For Elective SurgeryarchanaNessuna valutazione finora
- Jan LDeDocumento6 pagineJan LDearchanaNessuna valutazione finora
- Exercize ToleranceDocumento1 paginaExercize TolerancearchanaNessuna valutazione finora
- Melatonin in Humans - NEJMDocumento2 pagineMelatonin in Humans - NEJMarchanaNessuna valutazione finora
- Premedication With Melatonin Vs Midazolam in Anxious ChildrenDocumento2 paginePremedication With Melatonin Vs Midazolam in Anxious ChildrenarchanaNessuna valutazione finora
- Bone Cement and The Implications For AnaesthesiaDocumento6 pagineBone Cement and The Implications For AnaesthesiaarchanaNessuna valutazione finora
- Cardiovascular Exam GuideDocumento4 pagineCardiovascular Exam GuidearchanaNessuna valutazione finora
- Dijelovi Kuće-Radni ListićDocumento10 pagineDijelovi Kuće-Radni ListićGise Cerutti Pavić100% (1)
- AP Lit 2020 Test Study GuideDocumento3 pagineAP Lit 2020 Test Study GuideSusan ShankNessuna valutazione finora
- 3rd Monthly ExamDocumento4 pagine3rd Monthly ExamRoselyn PinionNessuna valutazione finora
- AQA-7131-7132-SP-2023Documento42 pagineAQA-7131-7132-SP-2023tramy.nguyenNessuna valutazione finora
- Current Trends On Assessment and EvaluationDocumento25 pagineCurrent Trends On Assessment and EvaluationDian Palupi100% (1)
- Examining Conflicts and Sharing Ideas in Panel DiscussionsDocumento4 pagineExamining Conflicts and Sharing Ideas in Panel DiscussionsOfficial Lara Delos SantosNessuna valutazione finora
- Jane Austen Persuasion Websters Korean Thesaurus Edition 2006 PDFDocumento291 pagineJane Austen Persuasion Websters Korean Thesaurus Edition 2006 PDFFLUENT TONGUENessuna valutazione finora
- Chem237LabManual Fall2012 RDocumento94 pagineChem237LabManual Fall2012 RKyle Tosh0% (1)
- F18Documento4 pagineF18Aayush ShahNessuna valutazione finora
- TLE 10 (Housekeeping) - Week 1 (Student's Copy)Documento2 pagineTLE 10 (Housekeeping) - Week 1 (Student's Copy)joel cagaananNessuna valutazione finora
- SteelDocumento23 pagineSteelMelinda GordonNessuna valutazione finora
- Psychiatric Mental Health Nursing CH 1Documento23 paginePsychiatric Mental Health Nursing CH 1sara75% (4)
- Lesson Plan 7e's Sea BreezeDocumento3 pagineLesson Plan 7e's Sea BreezeMark Joel Macaya GenoviaNessuna valutazione finora
- Transformacija Vojske Srbije PONOSScreen reader users, click here to turn off Google Instant. WebBooksShoppingVideosImagesMoreSearch tools About 119,000 results (0.37 seconds) Search Results Prokleta avlija - Wikipedia, slobodna enciklopedija ... sh.wikipedia.org/.../Proklet... Translate this pageSerbo‑Croatian Wikipedia U Andrićevoj noveli, Prokleta avlija je naziv poznate carigradske tamnice, u koju je iz neopravdanih razloga dospeo fra-Petar iz Bosne, koga su poslali u ... Radnja - Pripovedanje u prokletoj avliji - Višestruki naratori - Ekranizacija Ivo Andrić - Prokleta avlija prepričano lektira | Lektire.me www.lektire.me/.../ivo-andric-prokleta-avlija_21 Translate this page Pročitajte prepričavanje i detaljnu analizu književnog dela Ivo Andrić - Prokleta avlija. Prepričana lektira: Prokleta avlija - Ivo Andrić - Opušteno opusteno.rs › Diskusije › Književni kutak Translate this page Prepričana lektira: Prokleta avlija - Ivo Andrić Ivo Andrić – Prokleta avlija - kratak sadržajDocumento22 pagineTransformacija Vojske Srbije PONOSScreen reader users, click here to turn off Google Instant. WebBooksShoppingVideosImagesMoreSearch tools About 119,000 results (0.37 seconds) Search Results Prokleta avlija - Wikipedia, slobodna enciklopedija ... sh.wikipedia.org/.../Proklet... Translate this pageSerbo‑Croatian Wikipedia U Andrićevoj noveli, Prokleta avlija je naziv poznate carigradske tamnice, u koju je iz neopravdanih razloga dospeo fra-Petar iz Bosne, koga su poslali u ... Radnja - Pripovedanje u prokletoj avliji - Višestruki naratori - Ekranizacija Ivo Andrić - Prokleta avlija prepričano lektira | Lektire.me www.lektire.me/.../ivo-andric-prokleta-avlija_21 Translate this page Pročitajte prepričavanje i detaljnu analizu književnog dela Ivo Andrić - Prokleta avlija. Prepričana lektira: Prokleta avlija - Ivo Andrić - Opušteno opusteno.rs › Diskusije › Književni kutak Translate this page Prepričana lektira: Prokleta avlija - Ivo Andrić Ivo Andrić – Prokleta avlija - kratak sadržajGoran VukadinovicNessuna valutazione finora
- Lamm, J. Schleiermacher's PlatoDocumento278 pagineLamm, J. Schleiermacher's PlatonicodeloNessuna valutazione finora
- The Four Roles of A ReaderDocumento15 pagineThe Four Roles of A Readerapi-398545121Nessuna valutazione finora
- A Presentation of Gabriel Tarde and The End of SocialDocumento6 pagineA Presentation of Gabriel Tarde and The End of SocialHenrique Alcantara E SilvaNessuna valutazione finora
- From Observation To HypothesisDocumento2 pagineFrom Observation To HypothesiszkottNessuna valutazione finora
- Step-By-Step Analysis and Planning Guide: The Aira ApproachDocumento5 pagineStep-By-Step Analysis and Planning Guide: The Aira ApproachDaniel Osorio TorresNessuna valutazione finora
- Motivation LetterDocumento2 pagineMotivation Lettercho carl83% (18)
- Understanding Language VariationDocumento10 pagineUnderstanding Language VariationHesti AnandaNessuna valutazione finora
- Group CohesivenessDocumento26 pagineGroup CohesivenessRaviWadhawanNessuna valutazione finora
- Personal Position PaperDocumento18 paginePersonal Position Paperapi-258330934Nessuna valutazione finora
- Zero, First, and Second Conditional SentencesDocumento2 pagineZero, First, and Second Conditional SentencesAtzi EspinosaNessuna valutazione finora
- Introduction To Mass Communication Media Literacy and Culture 10th Edition Ebook PDF VersionDocumento62 pagineIntroduction To Mass Communication Media Literacy and Culture 10th Edition Ebook PDF Versionjames.brooks131100% (49)
- KPIsDocumento15 pagineKPIsbiswaksennayakNessuna valutazione finora
- Study Skills For SpellingDocumento2 pagineStudy Skills For Spellingapi-277816141Nessuna valutazione finora
- Pedo Long AnswerDocumento116 paginePedo Long AnswersamikshaNessuna valutazione finora
- Interview With Mitch Drazin Before and After EditingDocumento3 pagineInterview With Mitch Drazin Before and After Editingapi-285005584Nessuna valutazione finora
- Sptve Techdrwg7 Q1 M4Documento12 pagineSptve Techdrwg7 Q1 M4MarivicNovencidoNicolasNessuna valutazione finora
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionDa EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionValutazione: 4 su 5 stelle4/5 (402)
- Why We Die: The New Science of Aging and the Quest for ImmortalityDa EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityValutazione: 3.5 su 5 stelle3.5/5 (2)
- Outlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisDa EverandOutlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisValutazione: 4 su 5 stelle4/5 (1)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedDa EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedValutazione: 5 su 5 stelle5/5 (78)
- The Age of Magical Overthinking: Notes on Modern IrrationalityDa EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityValutazione: 4 su 5 stelle4/5 (13)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeDa EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeNessuna valutazione finora
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsDa EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsValutazione: 3.5 su 5 stelle3.5/5 (3)
- Techniques Exercises And Tricks For Memory ImprovementDa EverandTechniques Exercises And Tricks For Memory ImprovementValutazione: 4.5 su 5 stelle4.5/5 (40)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsDa EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsValutazione: 5 su 5 stelle5/5 (1)
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsDa EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsValutazione: 4.5 su 5 stelle4.5/5 (169)
- The Obesity Code: Unlocking the Secrets of Weight LossDa EverandThe Obesity Code: Unlocking the Secrets of Weight LossValutazione: 5 su 5 stelle5/5 (4)
- The Ultimate Guide To Memory Improvement TechniquesDa EverandThe Ultimate Guide To Memory Improvement TechniquesValutazione: 5 su 5 stelle5/5 (34)
- Roxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingDa EverandRoxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingValutazione: 5 su 5 stelle5/5 (4)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaDa EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaValutazione: 4.5 su 5 stelle4.5/5 (266)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsDa EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNessuna valutazione finora
- Summary: Limitless: Upgrade Your Brain, Learn Anything Faster, and Unlock Your Exceptional Life By Jim Kwik: Key Takeaways, Summary and AnalysisDa EverandSummary: Limitless: Upgrade Your Brain, Learn Anything Faster, and Unlock Your Exceptional Life By Jim Kwik: Key Takeaways, Summary and AnalysisValutazione: 5 su 5 stelle5/5 (8)
- Roxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingDa EverandRoxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingValutazione: 3.5 su 5 stelle3.5/5 (33)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Da EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Valutazione: 4.5 su 5 stelle4.5/5 (110)
- Summary: It Didn't Start with You: How Inherited Family Trauma Shapes Who We Are and How to End the Cycle By Mark Wolynn: Key Takeaways, Summary & AnalysisDa EverandSummary: It Didn't Start with You: How Inherited Family Trauma Shapes Who We Are and How to End the Cycle By Mark Wolynn: Key Takeaways, Summary & AnalysisValutazione: 5 su 5 stelle5/5 (3)
- The Happiness Trap: How to Stop Struggling and Start LivingDa EverandThe Happiness Trap: How to Stop Struggling and Start LivingValutazione: 4 su 5 stelle4/5 (1)
- The Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeDa EverandThe Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeValutazione: 4.5 su 5 stelle4.5/5 (253)
- The Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsDa EverandThe Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsNessuna valutazione finora
- The Tennis Partner: A Doctor's Story of Friendship and LossDa EverandThe Tennis Partner: A Doctor's Story of Friendship and LossValutazione: 4.5 su 5 stelle4.5/5 (4)