Potrebbero piacerti anche
- FinalDocumento1 paginaFinalKrisangela PasaolNessuna valutazione finora
- Scan 0001Documento1 paginaScan 0001Vishnu RamankuttyNessuna valutazione finora
- 1st Quarter Adopt A School ReportDocumento18 pagine1st Quarter Adopt A School ReportBaby PascuaNessuna valutazione finora
- Travel DivinaDocumento2 pagineTravel DivinaJames Lacuesta TabioloNessuna valutazione finora
- Classroom Daily Health Monitoring Tool For Covid-19: Grade 11-ChrysanthemumDocumento4 pagineClassroom Daily Health Monitoring Tool For Covid-19: Grade 11-Chrysanthemumkimbeerlyn doromasNessuna valutazione finora
- Department of Education: R II C V S D I J E DDocumento4 pagineDepartment of Education: R II C V S D I J E DElizabeth PelagioNessuna valutazione finora
- Division of Masbate: ClearanceDocumento1 paginaDivision of Masbate: ClearanceRhyz Mareschal DongonNessuna valutazione finora
- Graduation Program 2019 NEWDocumento10 pagineGraduation Program 2019 NEWdapitomaryjoyNessuna valutazione finora
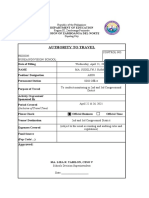
- Authority To Travel: Republic of The PhilippinesDocumento1 paginaAuthority To Travel: Republic of The PhilippinesFrederickVillaflorNessuna valutazione finora
- Huwag Mo PansininDocumento1 paginaHuwag Mo PansininMary May MatabangNessuna valutazione finora
- Ed169-Aquatic Camp 7Documento2 pagineEd169-Aquatic Camp 7api-643371905Nessuna valutazione finora
- Archbishop ColemanDocumento1 paginaArchbishop Colemanerykah722Nessuna valutazione finora
- Authority To Travel FormDocumento1 paginaAuthority To Travel FormJasmine Valenzuela TolosaNessuna valutazione finora
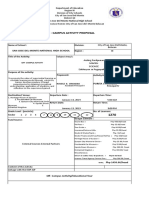
- Off - Campus Activity Proposal: San Jose Del Monte National High SchoolDocumento7 pagineOff - Campus Activity Proposal: San Jose Del Monte National High SchoolMa Lourdes MangahasNessuna valutazione finora
- New Authority To Travel (As of September 2019)Documento22 pagineNew Authority To Travel (As of September 2019)MAYLENE VILLAROSANessuna valutazione finora
- Sample PayrollDocumento6 pagineSample PayrollDeborah Fajardo ManabatNessuna valutazione finora
- Service Record: Department of EducationDocumento2 pagineService Record: Department of EducationAglanot ISNessuna valutazione finora
- 548 PTDP-NBC (Jun 27 To Jul 1,2022)Documento5 pagine548 PTDP-NBC (Jun 27 To Jul 1,2022)jhoanna cortezNessuna valutazione finora
- Division Travel Authority Revise Template 1 4Documento2 pagineDivision Travel Authority Revise Template 1 4JOEL D. BATERISNANessuna valutazione finora
- 03 Authority To TravelDocumento5 pagine03 Authority To TravelDiana Marie Vidallon AmanNessuna valutazione finora
- Authority To Travel: To Attend K-10 Training of Teachers (TOT) On Critical Content (Grade 7-MUSIC AND ARTSDocumento1 paginaAuthority To Travel: To Attend K-10 Training of Teachers (TOT) On Critical Content (Grade 7-MUSIC AND ARTSccmmcNessuna valutazione finora
- Bulacan: Dtyision of CityDocumento2 pagineBulacan: Dtyision of CityJethro Amcor MalaluanNessuna valutazione finora
- 1 2020 Deped Pang 2 HRD Form No 1 A Training Attendance Form For ParticipantsDocumento2 pagine1 2020 Deped Pang 2 HRD Form No 1 A Training Attendance Form For ParticipantsdeguiajericNessuna valutazione finora
- Itinerary of Travel Appendix BDocumento2 pagineItinerary of Travel Appendix Bfrederick.acosta01Nessuna valutazione finora
- Dianggal, Johair E.: Datu Ampanas Elementary School MAL E June 1, 2015Documento6 pagineDianggal, Johair E.: Datu Ampanas Elementary School MAL E June 1, 2015Mary Seal Cabrales-PejoNessuna valutazione finora
- Fees Shown Are Not To Be Charged To The Student But To CHED-Unifast ONLYDocumento1 paginaFees Shown Are Not To Be Charged To The Student But To CHED-Unifast ONLYSimple CottonNessuna valutazione finora
- Travel AuthorityDocumento2 pagineTravel AuthorityRobert Kier Tanquerido TomaroNessuna valutazione finora
- AUTHORITY TO TRAVEL For non-teachingDIVISION OFFICEDocumento7 pagineAUTHORITY TO TRAVEL For non-teachingDIVISION OFFICEBustamante N. RienalyNessuna valutazione finora
- Regional Director: Message of Dr. Isabelita M. Borres, Ceso IvDocumento10 pagineRegional Director: Message of Dr. Isabelita M. Borres, Ceso IvAlfredo Jr MallariNessuna valutazione finora
- Parents ConsentDocumento1 paginaParents ConsentShean Orvin BalaoNessuna valutazione finora
- Senior High School Student Permanent Record: Republic of The Philippines Department of EducationDocumento3 pagineSenior High School Student Permanent Record: Republic of The Philippines Department of EducationKENNEDY VAGAYNessuna valutazione finora
- DanicaDocumento15 pagineDanicaAndrian SasutilNessuna valutazione finora
- Republic of The Philippines Region IX, Zamboanga Peninsula Division of City Schools Minaog, Dipolog CityDocumento1 paginaRepublic of The Philippines Region IX, Zamboanga Peninsula Division of City Schools Minaog, Dipolog CityJustiniano CaermareNessuna valutazione finora
- Travel Order Seminar 2Documento1 paginaTravel Order Seminar 2Wilson CepeNessuna valutazione finora
- New Travel Order 2019 ALJOHN ESPLANADocumento4 pagineNew Travel Order 2019 ALJOHN ESPLANAaljohn esplanaNessuna valutazione finora
- 2020 Parents Consent Revised 2 1Documento12 pagine2020 Parents Consent Revised 2 1Gwyneth MarañaNessuna valutazione finora
- SAMPLE 2Documento26 pagineSAMPLE 2Edson Aljas LagudNessuna valutazione finora
- Fusion NotesDocumento2 pagineFusion NotesJohn Mark IndiongcoNessuna valutazione finora
- GF115 - Parent Permission Form ROPSAA 2023Documento2 pagineGF115 - Parent Permission Form ROPSAA 2023Priyanshi ChoksiNessuna valutazione finora
- 2023.03.25 TRA-03 Shipboard Education - Training.Drill Assessment Record - Heavy Weather DamageDocumento2 pagine2023.03.25 TRA-03 Shipboard Education - Training.Drill Assessment Record - Heavy Weather DamageFajar GemilangNessuna valutazione finora
- Authority To Travel: Republic of The Philippines Region IX, Zamboanga Peninsula Dipolog CityDocumento6 pagineAuthority To Travel: Republic of The Philippines Region IX, Zamboanga Peninsula Dipolog CityJoy SingsonNessuna valutazione finora
- Travel Order Prescrived For Out of DivisionDocumento1 paginaTravel Order Prescrived For Out of DivisionAldrin LabajoNessuna valutazione finora
- Student Recruitment and Retention: Building Capacity at MartinDocumento2 pagineStudent Recruitment and Retention: Building Capacity at MartinQuentin ThomasNessuna valutazione finora
- Learner'S Progress Report Card: Dipaculao National High SchoolDocumento3 pagineLearner'S Progress Report Card: Dipaculao National High SchoolRona Janoras GonzalesNessuna valutazione finora
- Applicants Documents ChecklistDocumento2 pagineApplicants Documents ChecklistLee Brenda PrecellasNessuna valutazione finora
- Travel OrderDocumento2 pagineTravel OrderRoger Cabarles IIINessuna valutazione finora
- Home Visit Plan and OthersDocumento12 pagineHome Visit Plan and OthersMariem Codilla AdoNessuna valutazione finora
- Activity Design 2Documento2 pagineActivity Design 2Onotan Chedjee Dods100% (1)
- Travel Order New TemplateDocumento11 pagineTravel Order New TemplateGenesis Terana-PerezNessuna valutazione finora
- 2019-2020 Adopt A School Program Report HsDocumento22 pagine2019-2020 Adopt A School Program Report HsJB RysNessuna valutazione finora
- Capitol University: Basic Education DepartmentDocumento3 pagineCapitol University: Basic Education DepartmentInah MeonadaNessuna valutazione finora
- School Form 7 (SF7) School Personnel Assignment List and Basic ProfileDocumento21 pagineSchool Form 7 (SF7) School Personnel Assignment List and Basic ProfileZeus SalazarNessuna valutazione finora
- Daily Attendance of VOlunteers BE 2019Documento1 paginaDaily Attendance of VOlunteers BE 2019Elisa Dela Reyna BaladadNessuna valutazione finora
- Central Mindanao University: Application FormDocumento2 pagineCentral Mindanao University: Application FormEdd Benedict B. DensingNessuna valutazione finora
- 2020 Coach Co Coach Chap DOCsDocumento4 pagine2020 Coach Co Coach Chap DOCsAlden Paceño100% (1)
- Online Learning Module Writing: Application FormDocumento3 pagineOnline Learning Module Writing: Application Formalvin n. vedarozagaNessuna valutazione finora
- GRADE XII (Semester 2) Page-6Documento2 pagineGRADE XII (Semester 2) Page-6Zainur RohmanNessuna valutazione finora
- Authority To Travel: Emeliano S. Fontanares Sr. National High SchoolDocumento6 pagineAuthority To Travel: Emeliano S. Fontanares Sr. National High SchoolDanica Cascabel LptNessuna valutazione finora
- Travel Order New FormatDocumento4 pagineTravel Order New FormatMae CortezNessuna valutazione finora
- Kevin Burns Meet and Greet April 10Documento1 paginaKevin Burns Meet and Greet April 10artounianNessuna valutazione finora
- ATM Event Announcement 011311Documento1 paginaATM Event Announcement 011311artounianNessuna valutazione finora
- MLK Candlelight Vigil 2011 FlyerDocumento1 paginaMLK Candlelight Vigil 2011 FlyerartounianNessuna valutazione finora
- Orientation Flyer Mourning HighDocumento2 pagineOrientation Flyer Mourning HighartounianNessuna valutazione finora
- Ti Bur On 2011 First SaleDocumento1 paginaTi Bur On 2011 First SaleartounianNessuna valutazione finora
- Need Help To Prepare For The SATDocumento2 pagineNeed Help To Prepare For The SATartounianNessuna valutazione finora
- 2010-2011 Membership Form EnglishDocumento2 pagine2010-2011 Membership Form EnglishartounianNessuna valutazione finora
- SummerreadinglistatmDocumento1 paginaSummerreadinglistatmartounianNessuna valutazione finora
- Math 7 Summative Test: - Read The Questions Carefully. Choose The Letter of Your Answer and Write It in YourDocumento4 pagineMath 7 Summative Test: - Read The Questions Carefully. Choose The Letter of Your Answer and Write It in Youretheljoy agpaoaNessuna valutazione finora
- CR 1993 Joyce ReynoldsDocumento2 pagineCR 1993 Joyce ReynoldsFlosquisMongisNessuna valutazione finora
- Hospitality Organizational ManagementDocumento16 pagineHospitality Organizational ManagementmikeltiongcoNessuna valutazione finora
- Salmonella Reflection PDFDocumento2 pagineSalmonella Reflection PDFcNessuna valutazione finora
- Sse 6115 Lesson Plan 5 Social Studies LessonDocumento4 pagineSse 6115 Lesson Plan 5 Social Studies Lessonapi-288702670Nessuna valutazione finora
- Preface of The Course File Lab-1 NewDocumento7 paginePreface of The Course File Lab-1 Newtheeppori_gctNessuna valutazione finora
- Interview Different TypesDocumento2 pagineInterview Different Typesআলটাফ হুছেইনNessuna valutazione finora
- EF3e Elem Filetest 12a Answer SheetDocumento1 paginaEF3e Elem Filetest 12a Answer SheetLígia LimaNessuna valutazione finora
- LipsDocumento6 pagineLipsSam WeaversNessuna valutazione finora
- MTB - Mle Lesson Plan November 6, 2023Documento3 pagineMTB - Mle Lesson Plan November 6, 2023sherry ann corderoNessuna valutazione finora
- Application Form SaumuDocumento4 pagineApplication Form SaumuSaumu AbdiNessuna valutazione finora
- Full-Time Salaried Employees: Salary by Career Stage: Base Salary Total RemunerationDocumento14 pagineFull-Time Salaried Employees: Salary by Career Stage: Base Salary Total RemunerationChuckbartowskiNessuna valutazione finora
- InclusionDocumento18 pagineInclusionmiha4adiNessuna valutazione finora
- Lovis Reji: Education SkillsDocumento2 pagineLovis Reji: Education SkillsLiya Mary VargheseNessuna valutazione finora
- Exam For Real Estate in CaliforniaDocumento230 pagineExam For Real Estate in Californiaharpay100% (9)
- School Health ServicesDocumento56 pagineSchool Health Servicessunielgowda80% (5)
- Liver Disease Management & TransplantDocumento4 pagineLiver Disease Management & TransplantMusike TeckneNessuna valutazione finora
- NITTTR PHD Within 7 YearsDocumento20 pagineNITTTR PHD Within 7 YearsFeroz IkbalNessuna valutazione finora
- Study Guide For Pipher Intro Chapter 1 Chapter 2Documento2 pagineStudy Guide For Pipher Intro Chapter 1 Chapter 2api-253671419Nessuna valutazione finora
- Lesson 1 Rizal 1Documento6 pagineLesson 1 Rizal 1Anne Maerick Jersey OteroNessuna valutazione finora
- Experts, Semantic and Epistemic: S G Northwestern UniversityDocumento18 pagineExperts, Semantic and Epistemic: S G Northwestern UniversityBrian BarreraNessuna valutazione finora
- The Wick: The Magazine of Hartwick College - Summer 2011Documento56 pagineThe Wick: The Magazine of Hartwick College - Summer 2011Stephanie BrunettaNessuna valutazione finora
- Program Assessment Tool Kit:: A Guide To Conducting Interviews and Surveys A Guide To Conducting Interviews and SurveysDocumento74 pagineProgram Assessment Tool Kit:: A Guide To Conducting Interviews and Surveys A Guide To Conducting Interviews and Surveyswinter55Nessuna valutazione finora
- Effects of Violent Online Games To Adolescent AggressivenessDocumento20 pagineEffects of Violent Online Games To Adolescent AggressivenesssorceressvampireNessuna valutazione finora
- Detailed Lesson Plan For DemoDocumento11 pagineDetailed Lesson Plan For DemoCheng ChengNessuna valutazione finora
- AssignmentB Step1 AdviceonAproachingThisAssignmentDocumento4 pagineAssignmentB Step1 AdviceonAproachingThisAssignmentOckert DavisNessuna valutazione finora
- Padagogy MathsDocumento344 paginePadagogy MathsRaju JagatiNessuna valutazione finora
- E-Portfolio: Noriza A. H. ShaariDocumento63 pagineE-Portfolio: Noriza A. H. ShaariNajikNessuna valutazione finora
- Modern Labor Economics: Inequality in EarningsDocumento37 pagineModern Labor Economics: Inequality in EarningssamuelNessuna valutazione finora
- Reyes Tag Ppt-PrefinalsDocumento11 pagineReyes Tag Ppt-PrefinalsRaphaella Mae Alegre ReyesNessuna valutazione finora