Potrebbero piacerti anche
- Seminar On Standing Orders and Protocols and Use of Selected Life SavingDocumento18 pagineSeminar On Standing Orders and Protocols and Use of Selected Life SavingmalathiNessuna valutazione finora
- On Standing OrderDocumento25 pagineOn Standing OrderPiyush Dutta100% (2)
- Preventive Obstetrics: Presented By-Itismita Biswal M, Sc. Nursing (1) Yr Obstetrics & Gynaecological NursingDocumento20 paginePreventive Obstetrics: Presented By-Itismita Biswal M, Sc. Nursing (1) Yr Obstetrics & Gynaecological NursingPabhat Kumar89% (9)
- Research Priorities in Obstetrics SeminarDocumento7 pagineResearch Priorities in Obstetrics SeminarSharmistha Debnath83% (6)
- Abortion Legislation inDocumento57 pagineAbortion Legislation inValarmathi Thangadurai100% (1)
- Seminar On Various Child Birth Practice, PositionDocumento26 pagineSeminar On Various Child Birth Practice, PositionPiyush Dutta100% (1)
- Recent Advancement in Contraceptive TechnologyDocumento3 pagineRecent Advancement in Contraceptive Technologyjeelani saima83% (6)
- 5174health Promotion Models in Midwifery - Raheega 3Documento54 pagine5174health Promotion Models in Midwifery - Raheega 3Jyoti Prem Uttam100% (3)
- Preventive Obstetrics PDFDocumento25 paginePreventive Obstetrics PDFAnju MargaretNessuna valutazione finora
- Evidence Based Practices in Obstetrical and Gynaecological NursingDocumento40 pagineEvidence Based Practices in Obstetrical and Gynaecological Nursingpratibhakamath97% (30)
- Preventive Obstetrics (By Mohan.s)Documento52 paginePreventive Obstetrics (By Mohan.s)mOHAN.S98% (55)
- Theories Applied To MidwiferyDocumento25 pagineTheories Applied To Midwiferybhawna82% (22)
- Seminar On Preventive ObstetricsDocumento49 pagineSeminar On Preventive ObstetricsRini Robert100% (3)
- Independent Nurse Midwifery PractitionerDocumento2 pagineIndependent Nurse Midwifery PractitionerShubhi Vaivhare100% (2)
- Annotated Bibliography of Obstretics & GynaecologyDocumento4 pagineAnnotated Bibliography of Obstretics & GynaecologyKaku ManishaNessuna valutazione finora
- On Epidemological Aspects of Maternal and Child HealthDocumento30 pagineOn Epidemological Aspects of Maternal and Child HealthBisma Maqbool67% (3)
- Magnitude of Maternal and Child Health ProblemsDocumento6 pagineMagnitude of Maternal and Child Health ProblemsKirandeep Parmar100% (6)
- Evidenced Based Midwifery PracticeDocumento23 pagineEvidenced Based Midwifery Practicepriyanka100% (4)
- Diagnostic Modalities in PregnancyDocumento11 pagineDiagnostic Modalities in PregnancyRavina Patel100% (1)
- Theories, Models in ObgDocumento83 pagineTheories, Models in ObgSyama Aneesh100% (1)
- Historical Perspectiv Obg NursingDocumento51 pagineHistorical Perspectiv Obg Nursingsutha71% (14)
- SYNOPSISDocumento25 pagineSYNOPSISpriyankaNessuna valutazione finora
- Manual Removal of PlacentaDocumento10 pagineManual Removal of PlacentaSanthosh.S.UNessuna valutazione finora
- Independent Nurse PractitionerDocumento14 pagineIndependent Nurse PractitionerKarishma Shroff100% (1)
- Epidermological Aspects of Meternal and Child Health Unit 1Documento24 pagineEpidermological Aspects of Meternal and Child Health Unit 1Pruthvi100% (4)
- Practice Standards For Obstetric and Gynaecological UnitDocumento27 paginePractice Standards For Obstetric and Gynaecological UnitRDi J100% (1)
- Puperium ComplicationDocumento75 paginePuperium Complicationvarshasharma05100% (1)
- Obg-Assignment On Family Welfare ServicesDocumento20 pagineObg-Assignment On Family Welfare ServicesRashmi C S75% (8)
- Effect of Drug During Pregnancy, Labour and PuerperiumDocumento10 pagineEffect of Drug During Pregnancy, Labour and PuerperiumSabeethu Girija63% (16)
- High Risk Approach in Maternal and Child HealthDocumento6 pagineHigh Risk Approach in Maternal and Child Healthjyotshna sahoo100% (5)
- MiesDocumento40 pagineMiessanthiyasandyNessuna valutazione finora
- Theories, Models and Approaches Applied To Midwifery PracticesDocumento111 pagineTheories, Models and Approaches Applied To Midwifery Practicesdr.anu Rk90% (10)
- Evidence Based Midwifery PracticeDocumento4 pagineEvidence Based Midwifery Practicesana naaz83% (6)
- National Policy and Legislation in Relation To Maternal Health and WelfareDocumento2 pagineNational Policy and Legislation in Relation To Maternal Health and WelfareKumar Suryavanshi89% (19)
- Surgical MenopauseDocumento12 pagineSurgical MenopausePabhat Kumar100% (1)
- SNCDocumento9 pagineSNCValarmathi100% (1)
- Problem Statement On Obstetric and Gynaecology: Name of GuideDocumento4 pagineProblem Statement On Obstetric and Gynaecology: Name of GuideAnita pataNessuna valutazione finora
- Assignment 1Documento9 pagineAssignment 1Lekshmi Manu69% (26)
- Seminar On National Health and Family Welfare Programmes Related To Maternal and ChildhealthDocumento21 pagineSeminar On National Health and Family Welfare Programmes Related To Maternal and ChildhealthKondapavuluru Jyothi81% (36)
- Seminar On Minor Ailments and Complications of PuerperiumDocumento74 pagineSeminar On Minor Ailments and Complications of PuerperiumKaruna Kumari89% (46)
- Role - of - Curriculum - Coordinator 3Documento8 pagineRole - of - Curriculum - Coordinator 3kamini Choudhary100% (1)
- Seminar On Theories, Models and Approaches Applied To Midwifery PracticeDocumento25 pagineSeminar On Theories, Models and Approaches Applied To Midwifery PracticeSANANessuna valutazione finora
- Fetal Measures PresentationDocumento6 pagineFetal Measures Presentationjeelani saima100% (1)
- Recent Advancement in Infertility Management and Adoption ProcessDocumento161 pagineRecent Advancement in Infertility Management and Adoption ProcessKripa Susan79% (24)
- Assignmenton Episiotomy CareDocumento5 pagineAssignmenton Episiotomy CarePriyaNessuna valutazione finora
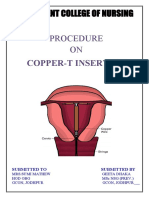
- Procedure ON: Copper-T InsertionDocumento5 pagineProcedure ON: Copper-T Insertionpriyanka100% (2)
- Dvance Ursing Ractice: Seminar ON Professional Organizations, Unions and Self DefenceDocumento19 pagineDvance Ursing Ractice: Seminar ON Professional Organizations, Unions and Self DefenceValarmathiNessuna valutazione finora
- B.usha Rani Dissertation Obg NursingDocumento224 pagineB.usha Rani Dissertation Obg Nursingabdullah khalid100% (1)
- Government College of Nursing Jodhpur: Procedure On-Cordocentesis Subject-Obstetrics & Gynecology Specialty-IDocumento4 pagineGovernment College of Nursing Jodhpur: Procedure On-Cordocentesis Subject-Obstetrics & Gynecology Specialty-Ipriyanka100% (2)
- Genetics and TeratologyDocumento21 pagineGenetics and Teratologypandem soniya0% (1)
- Various Childbirth PracticesDocumento11 pagineVarious Childbirth PracticesFarheen khan100% (1)
- Role and Scope ofDocumento18 pagineRole and Scope ofLekshmi Manu88% (33)
- Trends in The ObstetricsDocumento12 pagineTrends in The ObstetricssuthaNessuna valutazione finora
- National Family Welfare ProgramDocumento22 pagineNational Family Welfare ProgramAnuradha Maurya100% (9)
- Independent Nurse Practitioner 2Documento8 pagineIndependent Nurse Practitioner 2Krishnaveni Murugesh100% (3)
- Standing OrdersDocumento18 pagineStanding OrdersVijith.V.kumar78% (9)
- All India Institute of Medical Sciences Jodhpur College of Nursing Practice Teaching ONDocumento12 pagineAll India Institute of Medical Sciences Jodhpur College of Nursing Practice Teaching ONFarheen khanNessuna valutazione finora
- Emergency Tray PesentationDocumento14 pagineEmergency Tray Pesentationgaladimawa2002Nessuna valutazione finora
- Jawt 11 I 1 P 1Documento6 pagineJawt 11 I 1 P 1Jesicca SNessuna valutazione finora
- Organophosphate Poisoning 2Documento12 pagineOrganophosphate Poisoning 2Diana MurguiaNessuna valutazione finora
- Lesson Plan On Patterns of Nursing Education and Training Programmmes in IndiaDocumento15 pagineLesson Plan On Patterns of Nursing Education and Training Programmmes in Indiavarshasharma05Nessuna valutazione finora
- Female PelvisDocumento4 pagineFemale Pelvisvarshasharma05100% (1)
- Postpartum Hemorrhage FinalDocumento6 paginePostpartum Hemorrhage Finalvarshasharma05Nessuna valutazione finora
- Antenatal Care: Continuing Medical Education Activities For Non-Specialists DR TC Pun 27/2/2002Documento84 pagineAntenatal Care: Continuing Medical Education Activities For Non-Specialists DR TC Pun 27/2/2002tchale1Nessuna valutazione finora
- Lesson Plan On Collection of SpecimenDocumento3 pagineLesson Plan On Collection of Specimenvarshasharma0567% (3)
- First Page PDFDocumento1 paginaFirst Page PDFvarshasharma05Nessuna valutazione finora
- 3rd Stage of LabourDocumento22 pagine3rd Stage of Labourvarshasharma05100% (6)
- Menstrual CycleDocumento9 pagineMenstrual Cyclevarshasharma05100% (2)
- Female PelvisDocumento4 pagineFemale Pelvisvarshasharma05100% (1)
- Allcandidates Nurse 2Documento5.025 pagineAllcandidates Nurse 2varshasharma050% (1)
- Wa0001Documento8 pagineWa0001varshasharma05Nessuna valutazione finora
- Training Module Qualitative Research UpdatedDocumento4 pagineTraining Module Qualitative Research Updatedvarshasharma05Nessuna valutazione finora
- Handouts On Research Problem StatementDocumento2 pagineHandouts On Research Problem Statementvarshasharma05100% (1)
- COVID-19 Prevention & IEC Committee, PGIMER Chandigarh: Tentative Webinar Schedule For Healthcare ProfessionalsDocumento3 pagineCOVID-19 Prevention & IEC Committee, PGIMER Chandigarh: Tentative Webinar Schedule For Healthcare Professionalsvarshasharma05Nessuna valutazione finora
- Post B BSC Unit PlanDocumento3 paginePost B BSC Unit Planvarshasharma05100% (4)
- 160 Nursing Bullets: Medical-Surgical Nursing Reviewer: Nursing Diagnosis Care Plan NCLEX Questions Exam QuestionDocumento16 pagine160 Nursing Bullets: Medical-Surgical Nursing Reviewer: Nursing Diagnosis Care Plan NCLEX Questions Exam Questionvarshasharma05100% (4)
- Midwife MeansDocumento17 pagineMidwife Meansvarshasharma05Nessuna valutazione finora
- Lesson Plan On Eclampsia: Submitted To Mrs. Cimil Babu Assistant Professor Holi Family College of NursingDocumento13 pagineLesson Plan On Eclampsia: Submitted To Mrs. Cimil Babu Assistant Professor Holi Family College of Nursingvarshasharma0580% (5)
- 3rd Stage of Labour PDFDocumento15 pagine3rd Stage of Labour PDFvarshasharma05Nessuna valutazione finora
- Lesson Plan On Eclampsia: Submitted To Mrs. Cimil Babu Assistant Professor Holi Family College of NursingDocumento13 pagineLesson Plan On Eclampsia: Submitted To Mrs. Cimil Babu Assistant Professor Holi Family College of Nursingvarshasharma0580% (5)
- Notice No. 82 - NursingOfficerDocumento8 pagineNotice No. 82 - NursingOfficervarshasharma05Nessuna valutazione finora
- Baby Friendly Hospital Initiative and Exclusive Breast FeedingDocumento92 pagineBaby Friendly Hospital Initiative and Exclusive Breast Feedingvarshasharma05Nessuna valutazione finora
- 3rd Stage of Labour PDFDocumento15 pagine3rd Stage of Labour PDFvarshasharma05Nessuna valutazione finora
- Lesson Plan On PoliomyelitisDocumento12 pagineLesson Plan On Poliomyelitisvarshasharma05100% (1)
- Holy Family College of Nursing M.Sc. Nursing Second Year Obstetrics and Gynecology Master RotationDocumento2 pagineHoly Family College of Nursing M.Sc. Nursing Second Year Obstetrics and Gynecology Master Rotationvarshasharma05Nessuna valutazione finora
- Breastfeeding 120912050521 Phpapp01Documento57 pagineBreastfeeding 120912050521 Phpapp01varshasharma05Nessuna valutazione finora
- CareDocumento18 pagineCarevarshasharma05Nessuna valutazione finora
- Fire Safety ProtocolDocumento1 paginaFire Safety Protocolvarshasharma05Nessuna valutazione finora
- CommunicationDocumento23 pagineCommunicationvarshasharma05Nessuna valutazione finora
- Care of Low Birth Weight BabiesDocumento102 pagineCare of Low Birth Weight Babiesvarshasharma05100% (1)
- 101 Group Topics FinalDocumento1 pagina101 Group Topics FinalDavid J BrentNessuna valutazione finora
- Corona Kavach PolicyDocumento27 pagineCorona Kavach PolicyMichaelNessuna valutazione finora
- Proposal Bhalubang Community HospitalDocumento30 pagineProposal Bhalubang Community HospitalVenkat Ravichandran100% (3)
- Anaesthetic Considerations in Patients With Transverse MyelitisDocumento3 pagineAnaesthetic Considerations in Patients With Transverse MyelitisIniya RajendranNessuna valutazione finora
- Checklist Clinical Office Endos PDFDocumento20 pagineChecklist Clinical Office Endos PDFBABBY ZBOURGNessuna valutazione finora
- 670 1987 1 PBDocumento7 pagine670 1987 1 PBInal Banewa25Nessuna valutazione finora
- Drug Education PaperDocumento10 pagineDrug Education Paperapi-506661800Nessuna valutazione finora
- Congratulations To SendDocumento37 pagineCongratulations To SendLeslie Anne BiteNessuna valutazione finora
- The Integration LadderDocumento7 pagineThe Integration LadderTahir QaziNessuna valutazione finora
- Marketing and Advertising Casino Dealer Program 2Documento3 pagineMarketing and Advertising Casino Dealer Program 2Angela BrownNessuna valutazione finora
- Health Insurance in India-An Overview: K.Swathi, R.AnuradhaDocumento4 pagineHealth Insurance in India-An Overview: K.Swathi, R.AnuradhaAnkit YadavNessuna valutazione finora
- Gad 2023 Planning ConferenceDocumento15 pagineGad 2023 Planning ConferenceErnesto M FogataNessuna valutazione finora
- DKA-FBF2007-#04-Prometheus BooksDocumento71 pagineDKA-FBF2007-#04-Prometheus Booksapi-3766294100% (1)
- Material Safety Data Sheet Avapoly HTDocumento4 pagineMaterial Safety Data Sheet Avapoly HTfs1640Nessuna valutazione finora
- Entamoeba HistolyticaDocumento6 pagineEntamoeba HistolyticaWan Nur AnisaNessuna valutazione finora
- The Transition To Parenthood and MarriageDocumento9 pagineThe Transition To Parenthood and Marriageapi-534998120Nessuna valutazione finora
- Department of Education: Republic of The PhilippinesDocumento8 pagineDepartment of Education: Republic of The PhilippinesReysa m. DuatinNessuna valutazione finora
- Intensive Chi Kung CourseDocumento3 pagineIntensive Chi Kung CourseEdu TadeuNessuna valutazione finora
- ResearchDocumento71 pagineResearchAngeline Lareza-Reyna VillasorNessuna valutazione finora
- Persuasive Essay Sample For StudentsDocumento3 paginePersuasive Essay Sample For StudentsNathaniel SilotNessuna valutazione finora
- Acute Herpetic Gingivostomatitis Associated With Herpes Simplex Virus 2Documento4 pagineAcute Herpetic Gingivostomatitis Associated With Herpes Simplex Virus 2Ayu KartikaNessuna valutazione finora
- Benefit Verification Letter From The Social Security Administration For April 19 20Documento2 pagineBenefit Verification Letter From The Social Security Administration For April 19 20Shannon JaramilloNessuna valutazione finora
- Behavioral Skill TrainingDocumento28 pagineBehavioral Skill TrainingEttore CarloNessuna valutazione finora
- Surgical Nutrition: Vic V.Vernenkar, D.O. St. Barnabas Hospital Dept. of SurgeryDocumento54 pagineSurgical Nutrition: Vic V.Vernenkar, D.O. St. Barnabas Hospital Dept. of SurgeryAmir SharifNessuna valutazione finora
- Professional Disclosure StatementDocumento2 pagineProfessional Disclosure Statementapi-323266047Nessuna valutazione finora
- Malocclusion ArticleDocumento5 pagineMalocclusion Articlemeena syedNessuna valutazione finora
- Tren Dan Isue Water BirtDocumento14 pagineTren Dan Isue Water Birtijal_cakepNessuna valutazione finora
- HRM610 Final SlideDocumento19 pagineHRM610 Final SlideArju LubnaNessuna valutazione finora
- Final Exam Review NutritionDocumento9 pagineFinal Exam Review Nutritionjenm1228Nessuna valutazione finora
- Evaluation of Prosthetic Marginal Fit and Implant SurvivalDocumento12 pagineEvaluation of Prosthetic Marginal Fit and Implant SurvivalGustavo IsmaelNessuna valutazione finora