Potrebbero piacerti anche
- Use of Antibody Tests For SARS COV 2 in The Context of Digital Green CertificatesDocumento5 pagineUse of Antibody Tests For SARS COV 2 in The Context of Digital Green CertificatesFrancisca BallesterosNessuna valutazione finora
- Joint ECDC WHO Interim Advice On RCCE For Monkeypox 2 June 2022Documento7 pagineJoint ECDC WHO Interim Advice On RCCE For Monkeypox 2 June 2022Francisca BallesterosNessuna valutazione finora
- 3interim Advice For Public Health Authorities On Summer Events MPXDocumento6 pagine3interim Advice For Public Health Authorities On Summer Events MPXFrancisca BallesterosNessuna valutazione finora
- 5communicable Disease Threats Report 30 Jul 2022 PublicDocumento28 pagine5communicable Disease Threats Report 30 Jul 2022 PublicFrancisca BallesterosNessuna valutazione finora
- 2ECDC WHO Risk Communication Community Engagement Monkeypox Outbreak EuropeDocumento11 pagine2ECDC WHO Risk Communication Community Engagement Monkeypox Outbreak EuropeFrancisca BallesterosNessuna valutazione finora
- Interim Public Health Considerations For COVID 19 Vaccination of AdolescentsDocumento19 pagineInterim Public Health Considerations For COVID 19 Vaccination of AdolescentsFrancisca BallesterosNessuna valutazione finora
- Variable Dictionary VaccineTracker-04!11!2021Documento3 pagineVariable Dictionary VaccineTracker-04!11!2021Francisca BallesterosNessuna valutazione finora
- 1considerations For Contact Tracing MPX June 2022Documento13 pagine1considerations For Contact Tracing MPX June 2022Francisca BallesterosNessuna valutazione finora
- ROA Salmonella-Enteritidis-ST11 2022 FinalDocumento19 pagineROA Salmonella-Enteritidis-ST11 2022 FinalFrancisca BallesterosNessuna valutazione finora
- Agenda EAAD - European-Level Launch EventDocumento1 paginaAgenda EAAD - European-Level Launch EventFrancisca BallesterosNessuna valutazione finora
- Description and Disclaimer Daily ReportingDocumento1 paginaDescription and Disclaimer Daily ReportingFrancisca BallesterosNessuna valutazione finora
- COVID 19 in Children and The Role of School Settings in Transmission Second UpdateDocumento37 pagineCOVID 19 in Children and The Role of School Settings in Transmission Second UpdateFrancisca BallesterosNessuna valutazione finora
- COVID 19 Considerations For Booster Doses in Adolescents Feb 2022Documento14 pagineCOVID 19 Considerations For Booster Doses in Adolescents Feb 2022Francisca BallesterosNessuna valutazione finora
- 2021-01-13 Variable Dictionary and Disclaimer National Weekly DataDocumento1 pagina2021-01-13 Variable Dictionary and Disclaimer National Weekly DataFrancisca BallesterosNessuna valutazione finora
- Hiv and Aids: Surveillance ReportDocumento7 pagineHiv and Aids: Surveillance ReportFrancisca BallesterosNessuna valutazione finora
- Variable Dictionary VaccineTracker-20-08-2021Documento3 pagineVariable Dictionary VaccineTracker-20-08-2021Francisca BallesterosNessuna valutazione finora
- Communicable Disease Threats Report 16 Jun 2018Documento11 pagineCommunicable Disease Threats Report 16 Jun 2018Francisca BallesterosNessuna valutazione finora
- ECDC - Public Consultation - Expert Opinion On Rotavirus Vaccination in InfancyDocumento1 paginaECDC - Public Consultation - Expert Opinion On Rotavirus Vaccination in InfancyFrancisca BallesterosNessuna valutazione finora
- Antimicrobial Resistance Europe 2015Documento120 pagineAntimicrobial Resistance Europe 2015Francisca BallesterosNessuna valutazione finora
- Zika Virus Safety of Substances of Human Origin Update 2017 WebDocumento35 pagineZika Virus Safety of Substances of Human Origin Update 2017 WebFrancisca BallesterosNessuna valutazione finora
- Ecdc Infographics2015 Measles Is SeriousDocumento1 paginaEcdc Infographics2015 Measles Is SeriousFrancisca BallesterosNessuna valutazione finora
- Communicable Disease Threats Report 26 Aug 2017Documento9 pagineCommunicable Disease Threats Report 26 Aug 2017Francisca BallesterosNessuna valutazione finora
- Who Ccsivd Meetingreport SangreDocumento31 pagineWho Ccsivd Meetingreport SangreFrancisca BallesterosNessuna valutazione finora
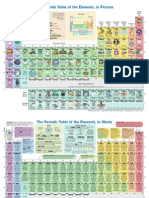
- The Periodic Table of Elements, in PicturesDocumento2 pagineThe Periodic Table of Elements, in Picturesrustyy88100% (1)
- ECDC - Systematic Review On Hepatitis B and C Prevalence in The EU-EEADocumento1 paginaECDC - Systematic Review On Hepatitis B and C Prevalence in The EU-EEAFrancisca BallesterosNessuna valutazione finora
- ECDC - ECDC Policy Briefing - Preparing For Zika in The EUDocumento1 paginaECDC - ECDC Policy Briefing - Preparing For Zika in The EUFrancisca BallesterosNessuna valutazione finora
- Communicable Disease Threats Report 29 Jul 2017Documento13 pagineCommunicable Disease Threats Report 29 Jul 2017Francisca BallesterosNessuna valutazione finora
- ECDC Policy BriefingsDocumento1 paginaECDC Policy BriefingsFrancisca BallesterosNessuna valutazione finora
- ECDC - Examples of Interventions To Manage Tuberculosis in Vulnerable GroupsDocumento2 pagineECDC - Examples of Interventions To Manage Tuberculosis in Vulnerable GroupsFrancisca BallesterosNessuna valutazione finora
- ECDC Epidemiological SituationDocumento1 paginaECDC Epidemiological SituationFrancisca BallesterosNessuna valutazione finora
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5794)
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (894)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (399)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (265)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (73)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (344)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (119)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- Relationship Analysis Between Leaf-Stomata CharactDocumento12 pagineRelationship Analysis Between Leaf-Stomata CharactTia AfridaNessuna valutazione finora
- Community Health Nursing ConceptsDocumento14 pagineCommunity Health Nursing Conceptssingireddi1revathi100% (2)
- COVID-19 Response Toolkit For New Mexico's Public SchoolsDocumento29 pagineCOVID-19 Response Toolkit For New Mexico's Public SchoolsErika EsquivelNessuna valutazione finora
- Treatment and Prevention of Enteric (Typhoid and Paratyphoid) Fever - UpToDate 2020Documento17 pagineTreatment and Prevention of Enteric (Typhoid and Paratyphoid) Fever - UpToDate 2020Zubair Mahmood KamalNessuna valutazione finora
- Virulence Genes Profile of Pseudomonas Aeruginosa Local Isolates From Burns and WoundsDocumento9 pagineVirulence Genes Profile of Pseudomonas Aeruginosa Local Isolates From Burns and WoundsZainab SattarNessuna valutazione finora
- CHN CS 5 PHC Services in OmanDocumento62 pagineCHN CS 5 PHC Services in OmanMelita Sheela AlvaNessuna valutazione finora
- VILSAN CatalougeDocumento97 pagineVILSAN CatalougeSầu VeNessuna valutazione finora
- Sample Registered Nurse Student ResumeDocumento25 pagineSample Registered Nurse Student ResumeAngela Camille100% (3)
- Why Do We Fall IllDocumento42 pagineWhy Do We Fall IllExabyteNessuna valutazione finora
- المختص في الحشرات -Synopsis of Medical EntomologyاDocumento63 pagineالمختص في الحشرات -Synopsis of Medical EntomologyاDrMohamedBenrashedNessuna valutazione finora
- Methodic Guidelines For Independent Preparation For Practical Classes For Applicants of Higher Medical Education in The 6-th Year of Study in The DisciplineDocumento68 pagineMethodic Guidelines For Independent Preparation For Practical Classes For Applicants of Higher Medical Education in The 6-th Year of Study in The DisciplineManav AryaNessuna valutazione finora
- tmpC737 TMPDocumento277 paginetmpC737 TMPFrontiersNessuna valutazione finora
- S521508004 PendahuluanDocumento13 pagineS521508004 Pendahuluanmasitah nasutionNessuna valutazione finora
- Practical Guidelines Infection Control PDFDocumento110 paginePractical Guidelines Infection Control PDFRao Rizwan Shakoor100% (1)
- Neonatal Sepsis: Ekawaty Lutfia Haksari Perinatology, Department of Child Health Gadjah Mada UniversityDocumento28 pagineNeonatal Sepsis: Ekawaty Lutfia Haksari Perinatology, Department of Child Health Gadjah Mada Universityireneaurelia100% (1)
- Short Report # 2017-07-529Documento8 pagineShort Report # 2017-07-529Raedah SaedehNessuna valutazione finora
- Epidemiology of Escherichia Coli Bacteremia: A Systematic Literature ReviewDocumento9 pagineEpidemiology of Escherichia Coli Bacteremia: A Systematic Literature ReviewMaria Chacón CarbajalNessuna valutazione finora
- Name: - Section: - Schedule: - Class Number: - DateDocumento5 pagineName: - Section: - Schedule: - Class Number: - DateAlbieRhioneilLatonioMacayanNessuna valutazione finora
- Emergency Care 13th Edition Limmer Test BankDocumento35 pagineEmergency Care 13th Edition Limmer Test Bankmichellesmith25081983ebo100% (23)
- Myco Viro Hand Out Batch2 UpdatedDocumento10 pagineMyco Viro Hand Out Batch2 UpdatedMark jay LlanoNessuna valutazione finora
- Sarla Birala BrochureDocumento18 pagineSarla Birala BrochurewithraviNessuna valutazione finora
- TNPSC - SYLLABUS - Veterinary Science (Code No.118)Documento2 pagineTNPSC - SYLLABUS - Veterinary Science (Code No.118)mobigangNessuna valutazione finora
- Extended Product Information Esha 2000supregsupDocumento3 pagineExtended Product Information Esha 2000supregsupGustavoNessuna valutazione finora
- TTH Edition 2nd EditionDocumento62 pagineTTH Edition 2nd EditionfrankcubeNessuna valutazione finora
- NCPs For ParotidectomyDocumento12 pagineNCPs For ParotidectomyCarla Manaloto50% (2)
- Characterization of Successful Root Canal TreatmenDocumento10 pagineCharacterization of Successful Root Canal TreatmenSitiRahmahAzharNessuna valutazione finora
- Paediatric Cardiac Surgical Antibiotic Prophylaxis: PurposeDocumento9 paginePaediatric Cardiac Surgical Antibiotic Prophylaxis: PurposeZamzam DomaNessuna valutazione finora
- AVDAP Full GuidelinesDocumento112 pagineAVDAP Full GuidelinesSnow HongNessuna valutazione finora
- Sociodemographic Characteristics of Patients With Advanced HIV Disease in Enugu, South-East Nigeria: A Retrospective Analysis of Program DataDocumento6 pagineSociodemographic Characteristics of Patients With Advanced HIV Disease in Enugu, South-East Nigeria: A Retrospective Analysis of Program DataInternational Journal of Innovative Science and Research TechnologyNessuna valutazione finora
- F2F MeaslesDocumento7 pagineF2F MeaslesMichelle Gliselle Guinto MallareNessuna valutazione finora