Potrebbero piacerti anche
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (400)
- Antidiabetes: Dr. Rachmat Hidayat Bagian Farmakologi Fakultas Kedokteran Universitas Sriwijaya 2012Documento20 pagineAntidiabetes: Dr. Rachmat Hidayat Bagian Farmakologi Fakultas Kedokteran Universitas Sriwijaya 2012real_septiady_madrid3532Nessuna valutazione finora
- Sticker GigiDocumento1 paginaSticker Gigireal_septiady_madrid3532Nessuna valutazione finora
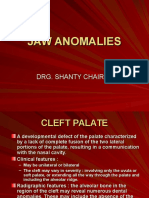
- Jaw AnomaliesDocumento12 pagineJaw AnomaliesyongkyNessuna valutazione finora
- GigikuDocumento1 paginaGigikureal_septiady_madrid3532Nessuna valutazione finora
- KeyfQUEJSOTDMR67835 PDFDocumento5 pagineKeyfQUEJSOTDMR67835 PDFreal_septiady_madrid3532Nessuna valutazione finora
- Buzzer JasmevDocumento1 paginaBuzzer Jasmevreal_septiady_madrid3532Nessuna valutazione finora
- Kelompok - 3Documento12 pagineKelompok - 3real_septiady_madrid3532Nessuna valutazione finora
- 167Documento9 pagine167real_septiady_madrid3532Nessuna valutazione finora
- Chapter 07 Apical Lesions - 2Documento25 pagineChapter 07 Apical Lesions - 2real_septiady_madrid3532Nessuna valutazione finora
- Pathway of The Pulp 10th EditionDocumento1 paginaPathway of The Pulp 10th Editionreal_septiady_madrid353225% (4)
- Epulis CronomarpologicalDocumento8 pagineEpulis CronomarpologicalPutri Ferina Aprilia SyaferiNessuna valutazione finora
- Epulis 000Documento2 pagineEpulis 000real_septiady_madrid3532Nessuna valutazione finora
- S R e T T R C VSP I T - Ar SDocumento5 pagineS R e T T R C VSP I T - Ar Sreal_septiady_madrid3532Nessuna valutazione finora
- 10Documento26 pagine10real_septiady_madrid3532Nessuna valutazione finora
- Obtura PackDocumento4 pagineObtura PackRedhabAbbassNessuna valutazione finora
- Studiu Dezinfectie AmprenteDocumento7 pagineStudiu Dezinfectie AmprenteJedai MikeNessuna valutazione finora
- Dugoni, Steven - Space Management in The Mixed DentitionDocumento11 pagineDugoni, Steven - Space Management in The Mixed Dentitionreal_septiady_madrid3532Nessuna valutazione finora
- T I: A B R S: HE Mpression Lueprint To Estorative UccessDocumento7 pagineT I: A B R S: HE Mpression Lueprint To Estorative Uccessreal_septiady_madrid3532Nessuna valutazione finora
- 130 M534Documento7 pagine130 M534Erna Karlinna D. YanthyNessuna valutazione finora
- Osseointegrated Dental Implants: Colonization and Antimicrobial SusceptibilityDocumento5 pagineOsseointegrated Dental Implants: Colonization and Antimicrobial Susceptibilityreal_septiady_madrid3532Nessuna valutazione finora
- Long Term Survival of Direct and Indirect Restorations Placed For The Treatment of Advanced Tooth WearDocumento5 pagineLong Term Survival of Direct and Indirect Restorations Placed For The Treatment of Advanced Tooth Wearreal_septiady_madrid3532Nessuna valutazione finora
- Juni Save Root Pulp J LSTR LDocumento6 pagineJuni Save Root Pulp J LSTR LAntony SebastianNessuna valutazione finora
- Bonded Reinforcing Materials For Esthetic Anterior Periodontal Tooth StabilizationDocumento2 pagineBonded Reinforcing Materials For Esthetic Anterior Periodontal Tooth Stabilizationbuggs1152Nessuna valutazione finora
- Caso Clinico ProtesiDocumento4 pagineCaso Clinico Protesireal_septiady_madrid3532Nessuna valutazione finora
- Vital SignDocumento6 pagineVital SignAlexanderbudi123Nessuna valutazione finora
- A Fixed Removable Partial Denture Treatment For Severe Ridge DefectDocumento7 pagineA Fixed Removable Partial Denture Treatment For Severe Ridge Defectreal_septiady_madrid3532Nessuna valutazione finora
- Table Respiration RateDocumento1 paginaTable Respiration Ratereal_septiady_madrid3532Nessuna valutazione finora
- Daftar Pustak1Documento3 pagineDaftar Pustak1real_septiady_madrid3532Nessuna valutazione finora
- Kam BingDocumento1 paginaKam Bingreal_septiady_madrid3532Nessuna valutazione finora
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (588)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (74)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (266)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (344)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (121)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- Gastrocnemius SoleusDocumento8 pagineGastrocnemius SoleusgoldfishxNessuna valutazione finora
- Anaesthetics Skills ChecklistDocumento16 pagineAnaesthetics Skills Checklistjeckleandjerry100% (1)
- Resume Jurnal ADocumento11 pagineResume Jurnal AannisaNessuna valutazione finora
- CalgaryDocumento44 pagineCalgaryGifuGifuNessuna valutazione finora
- Fasting Ramadan During PregnancyDocumento17 pagineFasting Ramadan During PregnancyHasiah Karim100% (1)
- 2nd Year Speciality MSNDocumento5 pagine2nd Year Speciality MSNJennifer DixonNessuna valutazione finora
- Hematology CasesDocumento27 pagineHematology Casessamkad214100% (2)
- Drkamalkv 1 Ans June-14Documento13 pagineDrkamalkv 1 Ans June-14Akshay MedkarNessuna valutazione finora
- NURS 366 Exam 1 Study Guide and RubricDocumento7 pagineNURS 366 Exam 1 Study Guide and RubriccmpNessuna valutazione finora
- Techniques in Family TherapyDocumento23 pagineTechniques in Family TherapyAntónio Martins100% (4)
- Ganglia: The Blackburn Foot and Ankle HyperbookDocumento3 pagineGanglia: The Blackburn Foot and Ankle Hyperbooksiddig7Nessuna valutazione finora
- Working With Mandated Substance Abusers - Language of SolutionsDocumento33 pagineWorking With Mandated Substance Abusers - Language of SolutionsbmckNessuna valutazione finora
- Hemo PathDocumento2 pagineHemo PathanadiguptaNessuna valutazione finora
- Program and Proceedings - 23rd International "STRESS AND BEHAVIOR" Neuroscience and Biopsychiatry Conference, St-Petersburg, Russia (May 16-19, 2016)Documento56 pagineProgram and Proceedings - 23rd International "STRESS AND BEHAVIOR" Neuroscience and Biopsychiatry Conference, St-Petersburg, Russia (May 16-19, 2016)ISBS_SocietyNessuna valutazione finora
- Nishi Symposium PresentationDocumento43 pagineNishi Symposium Presentationapi-231608392Nessuna valutazione finora
- Chap.30 Complications From Heart Disease WordDocumento6 pagineChap.30 Complications From Heart Disease WordcaisakiNessuna valutazione finora
- PRO Measures - Shoulder and Upper ExtremityDocumento27 paginePRO Measures - Shoulder and Upper ExtremityGonzalo QuiñonesNessuna valutazione finora
- Mind Control Forums - Complete Book ListDocumento11 pagineMind Control Forums - Complete Book ListSimon Benjamin100% (2)
- Gross Motor Development 6to12yearsDocumento17 pagineGross Motor Development 6to12yearsGul RockzzNessuna valutazione finora
- OsteosarcomaDocumento25 pagineOsteosarcomaChaitra Mahesh67% (3)
- Healthy Food PDFDocumento8 pagineHealthy Food PDFnurul syafizatul shahirahNessuna valutazione finora
- RSP Eit Booklet 9066788 en 2Documento152 pagineRSP Eit Booklet 9066788 en 2Panji NursetiaNessuna valutazione finora
- Healing Gardens FinalDocumento20 pagineHealing Gardens FinalMohd Salahuddin100% (1)
- DR Kumar Ponnusamy Biochemistry Genetics USMLE Preparatory Course BIOGEN Reusable On Line Resources For Large Group Teaching Learning in Relatively SHDocumento2 pagineDR Kumar Ponnusamy Biochemistry Genetics USMLE Preparatory Course BIOGEN Reusable On Line Resources For Large Group Teaching Learning in Relatively SHPonnusamy KumarNessuna valutazione finora
- Post Operative and Pre Prosthetic ManagementDocumento38 paginePost Operative and Pre Prosthetic ManagementTanzeelah RajawNessuna valutazione finora
- Night FeverDocumento5 pagineNight FeverdewioktaNessuna valutazione finora
- Rangkuman TeratomaDocumento22 pagineRangkuman TeratomaFelicia Fernanda IskandarNessuna valutazione finora
- NCP 1Documento4 pagineNCP 1Ke EjieNessuna valutazione finora
- Sialography ExaminationDocumento14 pagineSialography ExaminationEkaRahmaNessuna valutazione finora
- Is 2Documento10 pagineIs 2intan juitaNessuna valutazione finora