Potrebbero piacerti anche
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5794)
- Acute Upper Gastrointestinal Bleeding Acute Upper Gastrointestinal Bleeding OverviewDocumento11 pagineAcute Upper Gastrointestinal Bleeding Acute Upper Gastrointestinal Bleeding OverviewAnty Dewi Sarty RanyabarNessuna valutazione finora
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (399)
- AMC Recalls 2014Documento99 pagineAMC Recalls 2014saleema1175% (4)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- Calendar Printable A Little Pinch of Perfect PDFDocumento11 pagineCalendar Printable A Little Pinch of Perfect PDFSherah MayeNessuna valutazione finora
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (894)
- Hypoglycemia 508Documento12 pagineHypoglycemia 508saleema11Nessuna valutazione finora
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- Commonly Tested MRCP Part 1 Exam FactsDocumento3 pagineCommonly Tested MRCP Part 1 Exam Factssaleema11Nessuna valutazione finora
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
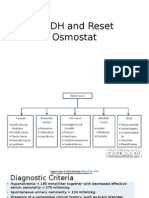
- SIADH and Reset OsmostatDocumento7 pagineSIADH and Reset Osmostatsaleema11Nessuna valutazione finora
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- Prostate screening, hypertension treatment, pregnancy complications, and psychiatric conditionsDocumento2 pagineProstate screening, hypertension treatment, pregnancy complications, and psychiatric conditionssaleema11Nessuna valutazione finora
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- Neeraj S Notes Step3Documento0 pagineNeeraj S Notes Step3Mrudula Rao100% (1)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (587)
- Dia Care 2015 Inzucchi 140 9Documento10 pagineDia Care 2015 Inzucchi 140 9Daniela MuñozNessuna valutazione finora
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (265)
- WHO DisasterDocumento26 pagineWHO Disastersaleema11Nessuna valutazione finora
- HyponatremiaDocumento10 pagineHyponatremiasaleema11Nessuna valutazione finora
- 1179 Full PDFDocumento10 pagine1179 Full PDFSonia RogersNessuna valutazione finora
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- TakafulDocumento1 paginaTakafulsaleema11Nessuna valutazione finora
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (73)
- Quiz Behavioral ScienceDocumento91 pagineQuiz Behavioral ScienceMedShare92% (12)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (344)
- Detect Metabolic Disorders Early with Laboratory TestsDocumento21 pagineDetect Metabolic Disorders Early with Laboratory Testssaleema11Nessuna valutazione finora
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- Quiz Behavioral ScienceDocumento91 pagineQuiz Behavioral ScienceMedShare92% (12)
- PsoriasisDocumento5 paginePsoriasissaleema11Nessuna valutazione finora
- WEEK 5 Management of Patients With Fluids and ElectrolytesDocumento89 pagineWEEK 5 Management of Patients With Fluids and ElectrolytesErica P. ManlunasNessuna valutazione finora
- Fluid and Electrolyte ImbalancesDocumento57 pagineFluid and Electrolyte ImbalancesTerry Mae Atilazal SarciaNessuna valutazione finora
- Goljan Notes by J. KurupDocumento41 pagineGoljan Notes by J. KurupBigz2222Nessuna valutazione finora
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- 1538 Exam 4 Cell Reg & GriefDocumento35 pagine1538 Exam 4 Cell Reg & GriefJade EdanoNessuna valutazione finora
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2219)
- NLE Questions )Documento6 pagineNLE Questions )galanzaloimar100% (2)
- Demeclocycline Effective for Treating SIADHDocumento4 pagineDemeclocycline Effective for Treating SIADHSally TareqNessuna valutazione finora
- Renal Function TestsDocumento23 pagineRenal Function TestsKer YehunNessuna valutazione finora
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- FULL-TEXT - NCLEX-RN Practice Quiz Test Bank 5 - NurseslabsDocumento77 pagineFULL-TEXT - NCLEX-RN Practice Quiz Test Bank 5 - NurseslabsRonaldo Matos PerezNessuna valutazione finora
- IM - Facts From Case Files CRCDocumento80 pagineIM - Facts From Case Files CRCridin007Nessuna valutazione finora
- Fluid and Electrolytes Made Insanely Easy PDFDocumento20 pagineFluid and Electrolytes Made Insanely Easy PDFCherry Ann Garcia Durante100% (7)
- Hyponatremia2010 (2014 - 09 - 24 18 - 08 - 47 UTC)Documento181 pagineHyponatremia2010 (2014 - 09 - 24 18 - 08 - 47 UTC)rnsharmasNessuna valutazione finora
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (119)
- Fluids and ElectrolytesDocumento15 pagineFluids and ElectrolytesTrisha UmaliNessuna valutazione finora
- EndocrinologyDocumento46 pagineEndocrinology[161]Shuaib AktherNessuna valutazione finora
- Hypertonic Saline 2018Documento3 pagineHypertonic Saline 2018Juan Esteban Soto DonosoNessuna valutazione finora
- Surgery Trans 2a - Fluid and Electrolyte Management of The Surgical PatientDocumento14 pagineSurgery Trans 2a - Fluid and Electrolyte Management of The Surgical PatientJoan Caacbay De GuzmanNessuna valutazione finora
- Siadh - Patho, Signs, Causes, TreatmentDocumento1 paginaSiadh - Patho, Signs, Causes, TreatmentVishalNessuna valutazione finora
- HyponatraemiaDocumento16 pagineHyponatraemiaRaluca LeucaNessuna valutazione finora
- NKL Review: Endocrine, GI, GU NursingDocumento6 pagineNKL Review: Endocrine, GI, GU NursingPaul ignacioNessuna valutazione finora
- Diabetes Insipidus and SIADH Reference Sheet: Normal Lab Values Siadh DIDocumento13 pagineDiabetes Insipidus and SIADH Reference Sheet: Normal Lab Values Siadh DIJohn TusselNessuna valutazione finora
- Hyponatremia Inpatient Management of JCG0342 V3Documento12 pagineHyponatremia Inpatient Management of JCG0342 V3zikryauliaNessuna valutazione finora
- CNS QuestionsDocumento39 pagineCNS QuestionsEvidence ChaibvaNessuna valutazione finora
- Hyponatremia in The Neurocritical Care PatientDocumento10 pagineHyponatremia in The Neurocritical Care PatientAli JENDOUBINessuna valutazione finora
- Top 40 Drugs and Nle FeedbacksDocumento106 pagineTop 40 Drugs and Nle FeedbacksGeraldin Buyagao KinlijanNessuna valutazione finora
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- Sample Final Year Exam - 2017Documento26 pagineSample Final Year Exam - 2017Taima FayezNessuna valutazione finora
- Fluids and Electrolytes2Documento8 pagineFluids and Electrolytes2Potchiee PfizerNessuna valutazione finora
- ScienceDocumento33 pagineScienceI am JNessuna valutazione finora
- Hyponatremia & Hypernatremia Quiz For NCLEX ExamDocumento1 paginaHyponatremia & Hypernatremia Quiz For NCLEX ExamNicole CansinoNessuna valutazione finora
- Endocrine Emergencies in PicuDocumento10 pagineEndocrine Emergencies in PicuDr.MohanNessuna valutazione finora
- Endocrine Problems of The Adult ClientDocumento18 pagineEndocrine Problems of The Adult ClientMarylle AntonioNessuna valutazione finora
- Last Minute Notes For USMLE Step 2CKDocumento16 pagineLast Minute Notes For USMLE Step 2CKJonathan B. Michaels100% (1)