Potrebbero piacerti anche
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5794)
- Finding Nutritive Value of Foodstuffs: How To Study This SectionDocumento15 pagineFinding Nutritive Value of Foodstuffs: How To Study This SectionDr-Jagadeesh MangamooriNessuna valutazione finora
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- JCMSDocumento6 pagineJCMSDr-Jagadeesh MangamooriNessuna valutazione finora
- Regional Meal Patterns: in ItDocumento23 pagineRegional Meal Patterns: in ItDr-Jagadeesh MangamooriNessuna valutazione finora
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- Finding Nutritive Value of Foodstuffs: How To Study This SectionDocumento15 pagineFinding Nutritive Value of Foodstuffs: How To Study This SectionDr-Jagadeesh MangamooriNessuna valutazione finora
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (895)
- Section 1 PDFDocumento30 pagineSection 1 PDFSanjeev Kumar SinghNessuna valutazione finora
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (344)
- Planning Diets I1: How To Study 'I'His SectionDocumento47 paginePlanning Diets I1: How To Study 'I'His SectionDr-Jagadeesh MangamooriNessuna valutazione finora
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (399)
- Nutrition DefinitionDocumento1 paginaNutrition DefinitionDr-Jagadeesh MangamooriNessuna valutazione finora
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (588)
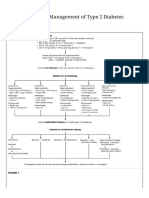
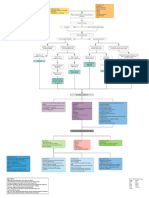
- Oral Agents in The Management of Type 2 Diabetes MellitusDocumento2 pagineOral Agents in The Management of Type 2 Diabetes MellitusDr-Jagadeesh MangamooriNessuna valutazione finora
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- Methods of Cooking: StudyDocumento11 pagineMethods of Cooking: StudyDr-Jagadeesh MangamooriNessuna valutazione finora
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (266)
- Pharm DDocumento8 paginePharm DDr-Jagadeesh MangamooriNessuna valutazione finora
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- Novel CORONA Virus StructureDocumento1 paginaNovel CORONA Virus StructureDr-Jagadeesh MangamooriNessuna valutazione finora
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- Medication ErrorsDocumento26 pagineMedication ErrorsDr-Jagadeesh Mangamoori75% (4)
- Oral Agents in The Management of Type 2 Diabetes MellitusDocumento2 pagineOral Agents in The Management of Type 2 Diabetes MellitusDr-Jagadeesh MangamooriNessuna valutazione finora
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (73)
- Nutrition and Food SystemsDocumento1 paginaNutrition and Food SystemsDr-Jagadeesh MangamooriNessuna valutazione finora
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- One-Way Analysis of Variance For Independent or Correlated SamplesDocumento4 pagineOne-Way Analysis of Variance For Independent or Correlated SamplesDr-Jagadeesh MangamooriNessuna valutazione finora
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- IGNOU Common Prospectus EnglishDocumento208 pagineIGNOU Common Prospectus Englishsanjibbhakta100% (1)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2259)
- DNHE Program GuideDocumento62 pagineDNHE Program GuideDr-Jagadeesh Mangamoori100% (1)
- Diagnosis of DKADocumento1 paginaDiagnosis of DKADr-Jagadeesh MangamooriNessuna valutazione finora
- NABH Hospitals ListDocumento36 pagineNABH Hospitals ListDr-Jagadeesh MangamooriNessuna valutazione finora
- Food Safety Officers Scheme Syllabus - APPSCDocumento4 pagineFood Safety Officers Scheme Syllabus - APPSCDr-Jagadeesh MangamooriNessuna valutazione finora
- WHO - SchizophreniaDocumento3 pagineWHO - SchizophreniaDr-Jagadeesh MangamooriNessuna valutazione finora
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- Anti ConvulsantDocumento3 pagineAnti ConvulsantDr-Jagadeesh MangamooriNessuna valutazione finora
- Query: SWINE FLU-Definition, Causes, Signs and Symptoms, Management? ResponseDocumento1 paginaQuery: SWINE FLU-Definition, Causes, Signs and Symptoms, Management? ResponseDr-Jagadeesh MangamooriNessuna valutazione finora
- IGNOU Common Prospectus EnglishDocumento208 pagineIGNOU Common Prospectus Englishsanjibbhakta100% (1)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- One-Way Analysis of Variance For Independent or Correlated SamplesDocumento4 pagineOne-Way Analysis of Variance For Independent or Correlated SamplesDr-Jagadeesh MangamooriNessuna valutazione finora
- Medication AdherenceDocumento36 pagineMedication AdherenceDr-Jagadeesh MangamooriNessuna valutazione finora
- Pediatric PoisoningDocumento47 paginePediatric PoisoningDr-Jagadeesh Mangamoori75% (4)
- Clinical PharmacyDocumento60 pagineClinical PharmacyDr-Jagadeesh MangamooriNessuna valutazione finora
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (120)
- Pediatric PoisoningDocumento47 paginePediatric PoisoningDr-Jagadeesh Mangamoori75% (4)
- Communication SkillsDocumento70 pagineCommunication SkillsDr-Jagadeesh MangamooriNessuna valutazione finora
- A New Leadership Curriculum: The Multiplication of IntelligenceDocumento4 pagineA New Leadership Curriculum: The Multiplication of IntelligenceGisele PhaloNessuna valutazione finora
- OB AssessmentDocumento3 pagineOB AssessmentJoshua D ParkerNessuna valutazione finora
- CMCRT Cardiac Surgery PDFDocumento11 pagineCMCRT Cardiac Surgery PDFSuraj PathakNessuna valutazione finora
- Case Analysis COLON CANCERDocumento4 pagineCase Analysis COLON CANCERBelle A. Basilio50% (2)
- Chronic Pain and PsychologyDocumento3 pagineChronic Pain and PsychologyOluwafemi OlarindeNessuna valutazione finora
- Poster-Youth Friendly SRH Services in SchoolsDocumento1 paginaPoster-Youth Friendly SRH Services in SchoolsApril Rose Airoso - AramburoNessuna valutazione finora
- Dermovate-NN Ointment: 1. What This Medicine Is and What It Is Used ForDocumento1 paginaDermovate-NN Ointment: 1. What This Medicine Is and What It Is Used ForIftikhar RasheedNessuna valutazione finora
- Rhinology Fellowship InfoDocumento2 pagineRhinology Fellowship InfoSabyasachi Chakrabarti100% (3)
- REFLECTION PE & HealthDocumento1 paginaREFLECTION PE & HealthPenelope CarandangNessuna valutazione finora
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- Ac 76583 Pfdqwertaf 79898 TseDocumento548 pagineAc 76583 Pfdqwertaf 79898 TseMerve EmelNessuna valutazione finora
- Rickettsial DiseasesDocumento44 pagineRickettsial DiseasesPrince AlexNessuna valutazione finora
- CURS - ENGLEZA - Boli Infectioase PDFDocumento246 pagineCURS - ENGLEZA - Boli Infectioase PDFLesan IulianaNessuna valutazione finora
- IARC CX Ca Screening PDFDocumento313 pagineIARC CX Ca Screening PDFderr barrNessuna valutazione finora
- Lesson 1 (His) - Reflective LearningDocumento1 paginaLesson 1 (His) - Reflective LearningCristina PitongNessuna valutazione finora
- Myocardial Infarction With CABG Concept MapDocumento1 paginaMyocardial Infarction With CABG Concept MapMaria Therese100% (1)
- Seminars in Diagnostic Pathology: Mark R. WickDocumento12 pagineSeminars in Diagnostic Pathology: Mark R. WickNancy ManriqueNessuna valutazione finora
- Senior Project Paper FinalDocumento5 pagineSenior Project Paper Finalapi-281742815Nessuna valutazione finora
- NCP Risk For FallsDocumento1 paginaNCP Risk For FallsMary Joyce71% (14)
- Hesi Altered NutritionDocumento8 pagineHesi Altered NutritionAna BienneNessuna valutazione finora
- General Form No 86 Health ExaminationDocumento1 paginaGeneral Form No 86 Health ExaminationArminda Annabelle Bangks86% (22)
- 1.1.2 OSH Foundations and Its Benefits - CEC 003-CEC32S6 - Construction Occupational Safety and Health (COSH)Documento4 pagine1.1.2 OSH Foundations and Its Benefits - CEC 003-CEC32S6 - Construction Occupational Safety and Health (COSH)RYAN JOSEPH QUIMONessuna valutazione finora
- 2021 ESC Guidelines For The Diagnosis and Treatment of Acute and Chronic Heart FailureDocumento137 pagine2021 ESC Guidelines For The Diagnosis and Treatment of Acute and Chronic Heart FailuredianNessuna valutazione finora
- Murottal and Clasical Music Therapy Reducing Pra Cardiac Chateterization AnxietyDocumento9 pagineMurottal and Clasical Music Therapy Reducing Pra Cardiac Chateterization AnxietyElsaNessuna valutazione finora
- The Summary of An Urdu Version of Diabetes Self-CaDocumento7 pagineThe Summary of An Urdu Version of Diabetes Self-CaYASIR HAMIDNessuna valutazione finora
- Sistim Pencitraan Kedokteran Nuklir: Nur Rahmah Hidayati, M.SCDocumento7 pagineSistim Pencitraan Kedokteran Nuklir: Nur Rahmah Hidayati, M.SCSalsabila LuvaridianNessuna valutazione finora
- Red EyeDocumento45 pagineRed EyeDavidVictoriousLukas100% (1)
- Department of Education: Learners' ProfileDocumento3 pagineDepartment of Education: Learners' ProfileJennifer TabaqueNessuna valutazione finora
- Activity 8 - 5 Issues in The PhilippinesDocumento3 pagineActivity 8 - 5 Issues in The PhilippinesChristel Mae BoseoNessuna valutazione finora
- PACU Monitoring Sheet - RR Record - SCT-CONDocumento4 paginePACU Monitoring Sheet - RR Record - SCT-CONFitz JaminitNessuna valutazione finora
- Developmental Stages of Social Emotional Development in ChildrenDocumento7 pagineDevelopmental Stages of Social Emotional Development in ChildrenMia DacuroNessuna valutazione finora
- Breaking the Habit of Being YourselfDa EverandBreaking the Habit of Being YourselfValutazione: 4.5 su 5 stelle4.5/5 (1458)
- Summary of Noah Kagan's Million Dollar WeekendDa EverandSummary of Noah Kagan's Million Dollar WeekendValutazione: 5 su 5 stelle5/5 (1)
- Summary of The 4-Hour Body: An Uncommon Guide to Rapid Fat-Loss, Incredible Sex, and Becoming Superhuman by Timothy FerrissDa EverandSummary of The 4-Hour Body: An Uncommon Guide to Rapid Fat-Loss, Incredible Sex, and Becoming Superhuman by Timothy FerrissValutazione: 4.5 su 5 stelle4.5/5 (81)
- How to Talk to Anyone at Work: 72 Little Tricks for Big Success Communicating on the JobDa EverandHow to Talk to Anyone at Work: 72 Little Tricks for Big Success Communicating on the JobValutazione: 4.5 su 5 stelle4.5/5 (36)
- The Coaching Habit: Say Less, Ask More & Change the Way You Lead ForeverDa EverandThe Coaching Habit: Say Less, Ask More & Change the Way You Lead ForeverValutazione: 4.5 su 5 stelle4.5/5 (186)