Potrebbero piacerti anche
- Best Practices of Apheresis in Hematopoietic Cell TransplantationDa EverandBest Practices of Apheresis in Hematopoietic Cell TransplantationSyed A. AbutalibNessuna valutazione finora
- Transfusion of ABO-mismatched Platelets Leads To Early Platelet RefractorinessDocumento6 pagineTransfusion of ABO-mismatched Platelets Leads To Early Platelet Refractorinessmy accountNessuna valutazione finora
- Indications For Platelet Transfusion in Children With Acute LeukemiaDocumento10 pagineIndications For Platelet Transfusion in Children With Acute LeukemiaAbidi HichemNessuna valutazione finora
- How I Use Platelet TransfusionsDocumento12 pagineHow I Use Platelet TransfusionstheriversongsNessuna valutazione finora
- Immature Platelet Fraction Measured On The Sysmex XNeDocumento7 pagineImmature Platelet Fraction Measured On The Sysmex XNetuanbu164Nessuna valutazione finora
- How I Use Platelet TransfusionsDocumento12 pagineHow I Use Platelet TransfusionsJovanna OrtuñoNessuna valutazione finora
- Blood - BLD 2022 016558 C MainDocumento12 pagineBlood - BLD 2022 016558 C MaincnshematologiaNessuna valutazione finora
- How I Use Platelet Transfusions - Blood 2022Documento12 pagineHow I Use Platelet Transfusions - Blood 2022Jessica FloresNessuna valutazione finora
- Advances 017699Documento9 pagineAdvances 017699Danang Bagus UntoroNessuna valutazione finora
- Algoritmo de Transfusion en Pacientes CardiologicosDocumento8 pagineAlgoritmo de Transfusion en Pacientes CardiologicosLyonTrioréNessuna valutazione finora
- Briggs2006 PDFDocumento10 pagineBriggs2006 PDFRonal WinterNessuna valutazione finora
- Blood in TraumaDocumento17 pagineBlood in TraumaEmtha SeeniNessuna valutazione finora
- 862 FullDocumento3 pagine862 FullFadel BilondatuNessuna valutazione finora
- Massive Transfusion ProtocolDocumento11 pagineMassive Transfusion ProtocolAlaa Abdelmoaty OmranNessuna valutazione finora
- The Misunderstood Coagulopathy of Liver Disease - WJM 2018Documento9 pagineThe Misunderstood Coagulopathy of Liver Disease - WJM 2018J doeNessuna valutazione finora
- Bloodproducttransfusions Andreactions: Jessica L. Osterman,, Sanjay AroraDocumento12 pagineBloodproducttransfusions Andreactions: Jessica L. Osterman,, Sanjay AroraAdi ParamarthaNessuna valutazione finora
- NIH Public Access: Author ManuscriptDocumento20 pagineNIH Public Access: Author ManuscriptSantiago PilataxiNessuna valutazione finora
- Platelet Transfusion: A Clinical Practice Guideline From The AABB FreeDocumento6 paginePlatelet Transfusion: A Clinical Practice Guideline From The AABB FreeUJI MUTUNessuna valutazione finora
- Activity No 2 ImmunohematologyDocumento3 pagineActivity No 2 ImmunohematologyAegina FestinNessuna valutazione finora
- Seminario 13 2014 PDFDocumento8 pagineSeminario 13 2014 PDFJuan Jose PereiraNessuna valutazione finora
- Yagmur Et Al 2013 Platelet Hyperaggregability Is Highly Prevalent in Patients With Chronic Kidney Disease AnDocumento7 pagineYagmur Et Al 2013 Platelet Hyperaggregability Is Highly Prevalent in Patients With Chronic Kidney Disease AnMister FannaniNessuna valutazione finora
- Chest Masive TransfDocumento16 pagineChest Masive TransfMacario Ismael Chavez CutzNessuna valutazione finora
- Risk Factors For Intraoperative Massive Transfusion in Pediatric Liver Transplantation: A Multivariate AnalysisDocumento8 pagineRisk Factors For Intraoperative Massive Transfusion in Pediatric Liver Transplantation: A Multivariate AnalysisSanti ParambangNessuna valutazione finora
- 5.6 TransfusionDocumento2 pagine5.6 TransfusionamandajaeNessuna valutazione finora
- Thrombocytopenia in Chronic Liver Disease: Lessons From Transplanted PatientsDocumento5 pagineThrombocytopenia in Chronic Liver Disease: Lessons From Transplanted PatientsElena CuibanNessuna valutazione finora
- Blood Transfusion in Critical Care: Giora Netzer, Richard P Dutton and John R HessDocumento3 pagineBlood Transfusion in Critical Care: Giora Netzer, Richard P Dutton and John R Hessnevermore11Nessuna valutazione finora
- Arteriovenous Thrombosis in Chronic Renal Failure Patients Receiving Renal Replacement TherapyDocumento6 pagineArteriovenous Thrombosis in Chronic Renal Failure Patients Receiving Renal Replacement TherapyMaya RustamNessuna valutazione finora
- Addison K May, MD John P Reilly, MD, Msce Scott Manaker, MD, PHD Arthur J Silvergleid, MD Geraldine Finlay, MD Contributor DisclosuresDocumento12 pagineAddison K May, MD John P Reilly, MD, Msce Scott Manaker, MD, PHD Arthur J Silvergleid, MD Geraldine Finlay, MD Contributor DisclosuresAlvaro HaroNessuna valutazione finora
- A Prospective Study To CorrelateDocumento6 pagineA Prospective Study To Correlateelaaannabi1Nessuna valutazione finora
- Platelet Transfusion TherapyDocumento3 paginePlatelet Transfusion TherapydrrdchauhanNessuna valutazione finora
- TransfusiDocumento10 pagineTransfusiDevia PebriyentiNessuna valutazione finora
- HP94 04 PredictingDocumento8 pagineHP94 04 PredictingSa 'ng WijayaNessuna valutazione finora
- Embolizare Splenica PartialaDocumento5 pagineEmbolizare Splenica PartialaElena CuibanNessuna valutazione finora
- Stationary Versus Agitated Storage of Whole Blood.6 PDFDocumento5 pagineStationary Versus Agitated Storage of Whole Blood.6 PDFAngel CallesNessuna valutazione finora
- Emboli ParuDocumento10 pagineEmboli Paruindry_purnamasariNessuna valutazione finora
- Blood Product Replacement For Postpartum HemorrhageDocumento13 pagineBlood Product Replacement For Postpartum HemorrhageEvelyn Yanet Facho BautistaNessuna valutazione finora
- CMQCC - Transfusion in Obstetric HemorrhageDocumento10 pagineCMQCC - Transfusion in Obstetric HemorrhageBerri RahmadhoniNessuna valutazione finora
- Jama Neal 2023 Ed 230070 1696973944.14124Documento2 pagineJama Neal 2023 Ed 230070 1696973944.14124Luz Elena ValderramaNessuna valutazione finora
- Management of Adult Patients With Persistent Idiopathic Thrombocytopenic Purpura Following Splenectomy - A Systematic Review - PDocumento2 pagineManagement of Adult Patients With Persistent Idiopathic Thrombocytopenic Purpura Following Splenectomy - A Systematic Review - PSimona Persida Fulgeanu SoficaruNessuna valutazione finora
- Eppley 2004 GF in PRP Using GPS SystemDocumento7 pagineEppley 2004 GF in PRP Using GPS SystemViviane KaramNessuna valutazione finora
- Massive Tranfusion Protocol: Oleh ErtigaDocumento13 pagineMassive Tranfusion Protocol: Oleh ErtigaAnonymous BQM9271ZXNessuna valutazione finora
- Frank 2019Documento15 pagineFrank 2019Oliver ArteagaNessuna valutazione finora
- Postpartum Hemorrhage With A Standardized Massive Transfusion ProtocolDocumento9 paginePostpartum Hemorrhage With A Standardized Massive Transfusion Protocolmedicinaun74100% (2)
- Survival After Transarterial Embolization For Spontaneous Ruptured Hepatocellular CarcinomaDocumento5 pagineSurvival After Transarterial Embolization For Spontaneous Ruptured Hepatocellular CarcinomaRollin SidaurukNessuna valutazione finora
- Heparin-Induced Thrombocytopenia,: Thrombosis, and HemorrhageDocumento5 pagineHeparin-Induced Thrombocytopenia,: Thrombosis, and HemorrhageAchmad HafirulNessuna valutazione finora
- Review of Current Transfusion Therapy and Blood Banking PracticesDocumento52 pagineReview of Current Transfusion Therapy and Blood Banking PracticesAmaranto SantosoNessuna valutazione finora
- Misra 2012Documento7 pagineMisra 2012Carlos RiquelmeNessuna valutazione finora
- Kjg066 02 06Documento8 pagineKjg066 02 06Nguyễn PhúcNessuna valutazione finora
- General: Anaemia & Blood Cell Transfusion in Critical IllnessDocumento1 paginaGeneral: Anaemia & Blood Cell Transfusion in Critical IllnessOlfiany Laurenzia PongohNessuna valutazione finora
- Article in Press: Age of Blood and Survival After Massive TransfusionDocumento5 pagineArticle in Press: Age of Blood and Survival After Massive TransfusionJosé BlasNessuna valutazione finora
- Cost-Effectiveness of Blood Transfusion and White Cell Reduction in Elective Colorectal SurgeryDocumento4 pagineCost-Effectiveness of Blood Transfusion and White Cell Reduction in Elective Colorectal Surgerymy accountNessuna valutazione finora
- Plasma Exchange For Heparin-Induced Thrombocytopenia: Is There Enough Evidence?Documento4 paginePlasma Exchange For Heparin-Induced Thrombocytopenia: Is There Enough Evidence?sayednourNessuna valutazione finora
- Curley 2018 Platelet Transfusion Threshols in NeonatesDocumento11 pagineCurley 2018 Platelet Transfusion Threshols in NeonatesEllya Latifah IlyasNessuna valutazione finora
- J Jamcollsurg 2013 01 004Documento8 pagineJ Jamcollsurg 2013 01 004Wanjak ChawaponchaiNessuna valutazione finora
- Jeffrey L Carson Restrictive or Liberal TransfusionDocumento11 pagineJeffrey L Carson Restrictive or Liberal Transfusionmiguel aghelNessuna valutazione finora
- 3144.full MoyamoyaDocumento8 pagine3144.full MoyamoyaDarren ZytkiewiczNessuna valutazione finora
- Platelet Count in Predicting Bleeding Complication After Elective Endoscopy in Children With Portal Hypertension and ThrombocytopeniaDocumento4 paginePlatelet Count in Predicting Bleeding Complication After Elective Endoscopy in Children With Portal Hypertension and ThrombocytopeniaMasri YaniNessuna valutazione finora
- Bloody Easy PDFDocumento164 pagineBloody Easy PDFJenny JeongNessuna valutazione finora
- Bloodbook 2017 660 PDFDocumento7 pagineBloodbook 2017 660 PDFSambit DashNessuna valutazione finora
- Annsurg00185 0122Documento6 pagineAnnsurg00185 0122Fajr MuzammilNessuna valutazione finora
- Acid-Base Tutorial - Strong Ion DifferenceDocumento3 pagineAcid-Base Tutorial - Strong Ion DifferenceFadel BilondatuNessuna valutazione finora
- 4-2-3-1 Wide ,, Gatling Project ,, The Invicible ,, 142 Goals in League - (Update)Documento8 pagine4-2-3-1 Wide ,, Gatling Project ,, The Invicible ,, 142 Goals in League - (Update)Fadel BilondatuNessuna valutazione finora
- 14 Artikel MetaDocumento6 pagine14 Artikel MetaFadel BilondatuNessuna valutazione finora
- 862 FullDocumento3 pagine862 FullFadel BilondatuNessuna valutazione finora
- Comprehensive Pediatric NephrologyDocumento3 pagineComprehensive Pediatric NephrologyFadel BilondatuNessuna valutazione finora
- Symptoms and Diagnosis - ADHD - NCBDDD - CDCDocumento4 pagineSymptoms and Diagnosis - ADHD - NCBDDD - CDCFadel BilondatuNessuna valutazione finora
- WHO Immunologic Classification For HIVDocumento1 paginaWHO Immunologic Classification For HIVFadel BilondatuNessuna valutazione finora
- Ucm 439476Documento1 paginaUcm 439476Fadel BilondatuNessuna valutazione finora
- Disinfectants: Exercise 4Documento11 pagineDisinfectants: Exercise 4Jake GerolagaNessuna valutazione finora
- StreptococciDocumento91 pagineStreptococciDr. Ashish JawarkarNessuna valutazione finora
- STR 2.4 - Specific Technical Requirements For Accreditation of Haematology LaboratoriesDocumento16 pagineSTR 2.4 - Specific Technical Requirements For Accreditation of Haematology LaboratoriesTauke SengNessuna valutazione finora
- Unit 5 Module 12 CombinedDocumento9 pagineUnit 5 Module 12 Combinedapi-293001217Nessuna valutazione finora
- Isolation of Pure CultureDocumento7 pagineIsolation of Pure CultureVignesh ReddyNessuna valutazione finora
- Study of Illness Condition: Assessment Organ Involved Normal Function Pathophysiology AnalysisDocumento2 pagineStudy of Illness Condition: Assessment Organ Involved Normal Function Pathophysiology Analysisahmad ryanNessuna valutazione finora
- Steps in Viral Pathogenesis-Lecture ThreeDocumento3 pagineSteps in Viral Pathogenesis-Lecture ThreeIM CTNessuna valutazione finora
- Rocky Mountain Spotted Fever: Breeana Bardill Microbiology 429 LabDocumento22 pagineRocky Mountain Spotted Fever: Breeana Bardill Microbiology 429 LabbNessuna valutazione finora
- MLT ValidationDocumento3 pagineMLT Validationdeepanmb007100% (1)
- Streptococci and Enterococci and OthersDocumento11 pagineStreptococci and Enterococci and OthersthedarkwingNessuna valutazione finora
- Culture Characteristics of Common OrganismsDocumento5 pagineCulture Characteristics of Common OrganismssaketNessuna valutazione finora
- Probiotics in AquacultureDocumento7 pagineProbiotics in AquaculturemoiNessuna valutazione finora
- Nosocomial Infections in Pediatric Intensive Care UnitDocumento6 pagineNosocomial Infections in Pediatric Intensive Care UnitEditor IJTSRDNessuna valutazione finora
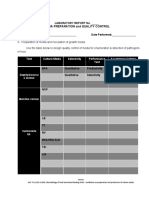
- Media Preparation and Quality ControlDocumento3 pagineMedia Preparation and Quality ControlclairealbertiniNessuna valutazione finora
- Controlling Microbial Growth in Vivo Using Antimicrobial AgentsDocumento30 pagineControlling Microbial Growth in Vivo Using Antimicrobial AgentsJen PanganibanNessuna valutazione finora
- Introduction To MicrobiologyDocumento55 pagineIntroduction To Microbiologymeldestacamentojr100% (3)
- Bacterial Contamination of Multiple-DoseDocumento5 pagineBacterial Contamination of Multiple-DoseMuhammad HabibieNessuna valutazione finora
- DarahDocumento14 pagineDarahChristantya VitaNessuna valutazione finora
- Foundations in Microbiology: TalaroDocumento71 pagineFoundations in Microbiology: Talaromertx013Nessuna valutazione finora
- Industrial Importance of MicrobesDocumento23 pagineIndustrial Importance of MicrobesDiah AyuningrumNessuna valutazione finora
- Prompt Inoculation System-D-3251-3000 PDFDocumento40 paginePrompt Inoculation System-D-3251-3000 PDFbogdan.tomosNessuna valutazione finora
- Multiple AllelesDocumento14 pagineMultiple AllelesSabs100% (2)
- Group 6 Blood Analysis 2Documento6 pagineGroup 6 Blood Analysis 2Kim TangoNessuna valutazione finora
- Lab 5 Coombs TestsDocumento26 pagineLab 5 Coombs TestsJennifer DixonNessuna valutazione finora
- DR Zalina - Trafusion Reaction and Management PDFDocumento77 pagineDR Zalina - Trafusion Reaction and Management PDFvasu_5iveNessuna valutazione finora
- SPREad PlateDocumento7 pagineSPREad PlateJermeLou BaoNessuna valutazione finora
- Immunohematology & Transfusion Medicine FinalDocumento33 pagineImmunohematology & Transfusion Medicine FinalCollen Mae Silos Diapues100% (1)
- Test Report: Complete Blood Count (CBC)Documento3 pagineTest Report: Complete Blood Count (CBC)WSC ALMANessuna valutazione finora
- Use This Form BLANK Blood Monitoring Report From RVBSPDocumento21 pagineUse This Form BLANK Blood Monitoring Report From RVBSPBadjoy Arcilla Dollente-ParialNessuna valutazione finora
- Study of Drug Resistance in Bacteria Using AntibiotiDocumento10 pagineStudy of Drug Resistance in Bacteria Using AntibiotiAshwin Rockzz75% (4)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedDa EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedValutazione: 4.5 su 5 stelle4.5/5 (82)
- ADHD is Awesome: A Guide to (Mostly) Thriving with ADHDDa EverandADHD is Awesome: A Guide to (Mostly) Thriving with ADHDValutazione: 5 su 5 stelle5/5 (4)
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionDa EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionValutazione: 4 su 5 stelle4/5 (404)
- Love Life: How to Raise Your Standards, Find Your Person, and Live Happily (No Matter What)Da EverandLove Life: How to Raise Your Standards, Find Your Person, and Live Happily (No Matter What)Valutazione: 3 su 5 stelle3/5 (1)
- The Age of Magical Overthinking: Notes on Modern IrrationalityDa EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityValutazione: 4 su 5 stelle4/5 (35)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsDa EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNessuna valutazione finora
- The Twentysomething Treatment: A Revolutionary Remedy for an Uncertain AgeDa EverandThe Twentysomething Treatment: A Revolutionary Remedy for an Uncertain AgeValutazione: 4.5 su 5 stelle4.5/5 (2)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsDa EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsValutazione: 4 su 5 stelle4/5 (5)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeDa EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeValutazione: 2 su 5 stelle2/5 (1)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Da EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Valutazione: 4.5 su 5 stelle4.5/5 (110)
- Cult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryDa EverandCult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryValutazione: 4 su 5 stelle4/5 (46)
- The Obesity Code: Unlocking the Secrets of Weight LossDa EverandThe Obesity Code: Unlocking the Secrets of Weight LossValutazione: 4 su 5 stelle4/5 (6)
- To Explain the World: The Discovery of Modern ScienceDa EverandTo Explain the World: The Discovery of Modern ScienceValutazione: 3.5 su 5 stelle3.5/5 (51)
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsDa EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsValutazione: 4.5 su 5 stelle4.5/5 (170)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaDa EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaValutazione: 4.5 su 5 stelle4.5/5 (266)
- The Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsDa EverandThe Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsNessuna valutazione finora
- The Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeDa EverandThe Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeValutazione: 4.5 su 5 stelle4.5/5 (254)
- Critical Thinking: How to Effectively Reason, Understand Irrationality, and Make Better DecisionsDa EverandCritical Thinking: How to Effectively Reason, Understand Irrationality, and Make Better DecisionsValutazione: 4.5 su 5 stelle4.5/5 (39)
- Summary: Limitless: Upgrade Your Brain, Learn Anything Faster, and Unlock Your Exceptional Life By Jim Kwik: Key Takeaways, Summary and AnalysisDa EverandSummary: Limitless: Upgrade Your Brain, Learn Anything Faster, and Unlock Your Exceptional Life By Jim Kwik: Key Takeaways, Summary and AnalysisValutazione: 5 su 5 stelle5/5 (8)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsDa EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsValutazione: 5 su 5 stelle5/5 (1)
- Manipulation: The Ultimate Guide To Influence People with Persuasion, Mind Control and NLP With Highly Effective Manipulation TechniquesDa EverandManipulation: The Ultimate Guide To Influence People with Persuasion, Mind Control and NLP With Highly Effective Manipulation TechniquesValutazione: 4.5 su 5 stelle4.5/5 (1412)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisDa EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisValutazione: 4.5 su 5 stelle4.5/5 (44)