Potrebbero piacerti anche
- Ben SonDocumento5 pagineBen SonDian NovitasariNessuna valutazione finora
- Arch Dis Child Fetal Neonatal Ed-2005 5876Documento6 pagineArch Dis Child Fetal Neonatal Ed-2005 5876Dian NovitasariNessuna valutazione finora
- Basics of Practical Genetics: Workbook I Course International Medical Faculty GroupDocumento16 pagineBasics of Practical Genetics: Workbook I Course International Medical Faculty GroupNehaNessuna valutazione finora
- Angelman SyndromeDocumento4 pagineAngelman SyndromeRowena DigalNessuna valutazione finora
- Common Dysmorphic Syndromes in The NICUDocumento12 pagineCommon Dysmorphic Syndromes in The NICUDaniel PuertasNessuna valutazione finora
- Reading Scholarly & Popular Sources on Autism StudyDocumento3 pagineReading Scholarly & Popular Sources on Autism StudyNishat MamnoonNessuna valutazione finora
- Reyes - Unit 2 (Part 2)Documento4 pagineReyes - Unit 2 (Part 2)Justine Ericca ReyesNessuna valutazione finora
- Congenital Hyperinsulinism: A Practical Guide to Diagnosis and ManagementDa EverandCongenital Hyperinsulinism: A Practical Guide to Diagnosis and ManagementDiva D. De León-CrutchlowNessuna valutazione finora
- Summary & Study Guide - The Gene Machine: How Genetic Technologies Are Changing the Way We Have Kids - and the Kids We HaveDa EverandSummary & Study Guide - The Gene Machine: How Genetic Technologies Are Changing the Way We Have Kids - and the Kids We HaveValutazione: 5 su 5 stelle5/5 (1)
- Moebius Sequence - A Multidisciplinary Clinical Approach: Research Open AccessDocumento11 pagineMoebius Sequence - A Multidisciplinary Clinical Approach: Research Open Accessfarah azizahNessuna valutazione finora
- CnsDocumento15 pagineCnsArun GeorgeNessuna valutazione finora
- (Osborn) Chapter 11: Learning Objectives (Number and Title)Documento22 pagine(Osborn) Chapter 11: Learning Objectives (Number and Title)KittiesNessuna valutazione finora
- Down Syndrome Diagnosis, Risk Factors and ManagementDocumento74 pagineDown Syndrome Diagnosis, Risk Factors and Managementanumeha sharma100% (2)
- Special Needs PopulationDocumento13 pagineSpecial Needs PopulationVina EmpialesNessuna valutazione finora
- Genetic TestingDocumento18 pagineGenetic Testingneha100% (1)
- Down syndrome screening resultsDocumento11 pagineDown syndrome screening resultslightning proNessuna valutazione finora
- Articol 1Documento7 pagineArticol 1nistor97Nessuna valutazione finora
- Childhood IllnessDocumento32 pagineChildhood IllnessJesseNessuna valutazione finora
- Angleman SyndromeDocumento9 pagineAngleman Syndromesongs semoNessuna valutazione finora
- Gratification Disorder ( Infantile Masturbation'') : A ReviewDocumento2 pagineGratification Disorder ( Infantile Masturbation'') : A ReviewGibran UsamahNessuna valutazione finora
- Review: Autism Spectrum Disorder: Advances in Evidence-Based PracticeDocumento11 pagineReview: Autism Spectrum Disorder: Advances in Evidence-Based PracticeWafaNessuna valutazione finora
- Alwahab2017 Article OccipitalMeningoencephaloceleC PDFDocumento4 pagineAlwahab2017 Article OccipitalMeningoencephaloceleC PDFOvamelia JulioNessuna valutazione finora
- Practica Basada en Lae Evidencia TEADocumento11 paginePractica Basada en Lae Evidencia TEAdadamianiNessuna valutazione finora
- Protocol EnglishDocumento1 paginaProtocol EnglishAdrian TaviNessuna valutazione finora
- 'OET' SAMPLE READING NEW DR TANJIM OVEE 2020Documento19 pagine'OET' SAMPLE READING NEW DR TANJIM OVEE 2020AHMED TANJIMUL ISLAMNessuna valutazione finora
- Scientists Discover Genetic Defect Responsible FoDocumento3 pagineScientists Discover Genetic Defect Responsible Foaestheticbambam3Nessuna valutazione finora
- AmniocentesisDocumento15 pagineAmniocentesisGYPSY CAT100% (1)
- Autism Spectrum DisorderDocumento4 pagineAutism Spectrum DisorderParishna BhuyanNessuna valutazione finora
- Ileal-lymphoid-nodular hyperplasia, non-specific colitis, and pervasive developmental disorder in childrenDocumento11 pagineIleal-lymphoid-nodular hyperplasia, non-specific colitis, and pervasive developmental disorder in childrenEmmanuelLeidiNessuna valutazione finora
- Munchausen's by ProxyDocumento7 pagineMunchausen's by ProxyAbdul-Kareem Ahmed100% (1)
- TMP FDE0Documento5 pagineTMP FDE0FrontiersNessuna valutazione finora
- Case Report For Case Presentations Short Rib Polydactyly SyndromeDocumento8 pagineCase Report For Case Presentations Short Rib Polydactyly Syndromeapi-390240132Nessuna valutazione finora
- Loss of The N-Myc Oncogene in A Patient With A Small Interstitial Deletion of The Short Arm of ChromosomeDocumento5 pagineLoss of The N-Myc Oncogene in A Patient With A Small Interstitial Deletion of The Short Arm of ChromosomeantonioopNessuna valutazione finora
- Diagnostic Exome Sequencing in Persons With Severe Intellectual DisabilityDocumento9 pagineDiagnostic Exome Sequencing in Persons With Severe Intellectual DisabilityMiaNessuna valutazione finora
- Genomes: What Makes Up A GenomeDocumento8 pagineGenomes: What Makes Up A GenomeDaniel BerryNessuna valutazione finora
- Vascular Limb Occlusion in Twin To Twin Tranfusion SyndromeDocumento10 pagineVascular Limb Occlusion in Twin To Twin Tranfusion Syndromejhon heriansyahNessuna valutazione finora
- Test Bank Maternal Child Nursing Care Womens Health 2nd Edition Ward HisleyDocumento28 pagineTest Bank Maternal Child Nursing Care Womens Health 2nd Edition Ward Hisleyjeremiahhartfozxmbqayn100% (15)
- Subconj Hemorrhage and AbuseDocumento5 pagineSubconj Hemorrhage and AbuseNurul Annisa muthaharaNessuna valutazione finora
- Deletion and Gain of Copies Variations Associated With Childhood Onset Psychosis Was YetDocumento5 pagineDeletion and Gain of Copies Variations Associated With Childhood Onset Psychosis Was YetAnonymous AY6XDZHBxPNessuna valutazione finora
- Ref 4Documento13 pagineRef 4Tiago BaraNessuna valutazione finora
- Disease Description Chromosomes On Which Known Loci Are LocatedDocumento4 pagineDisease Description Chromosomes On Which Known Loci Are Locatedapi-19641337Nessuna valutazione finora
- Munchausen Syndrome by ProxyDocumento8 pagineMunchausen Syndrome by ProxyClarissa YudakusumaNessuna valutazione finora
- The Influence of Heredity and Environment On Human DevelopmentDocumento48 pagineThe Influence of Heredity and Environment On Human DevelopmentShahrul FadreenNessuna valutazione finora
- Maternal Child Nursing Care 2nd Edition Ward Test BankDocumento28 pagineMaternal Child Nursing Care 2nd Edition Ward Test Bankalicenhan5bzm2z100% (32)
- Test Bank For Medical Genetics 4th Edition Lynn B JordeDocumento8 pagineTest Bank For Medical Genetics 4th Edition Lynn B JorderoytuyenbauNessuna valutazione finora
- Long Term Outcome of Small Versus Appropriate Size For Gestational Age Co-Twins/tripletsDocumento5 pagineLong Term Outcome of Small Versus Appropriate Size For Gestational Age Co-Twins/tripletsBerryEkaPardaBancinNessuna valutazione finora
- Microsoft Word - Genetic Disorders and PharmacogeneticsDocumento4 pagineMicrosoft Word - Genetic Disorders and PharmacogeneticsAmmar MashalyNessuna valutazione finora
- Human Chromosomal AbnormalitiesDocumento3 pagineHuman Chromosomal AbnormalitiescindyNessuna valutazione finora
- Study Chromosomes Cell Division KaryotypeDocumento4 pagineStudy Chromosomes Cell Division KaryotypeCerebrus GallantNessuna valutazione finora
- New Born Children With Encephalocele: Imedpub JournalsDocumento4 pagineNew Born Children With Encephalocele: Imedpub Journalsglory haurissaNessuna valutazione finora
- Neuroanatomy of Down's Syndrome: A High-Resolution MRI StudyDocumento7 pagineNeuroanatomy of Down's Syndrome: A High-Resolution MRI StudynananascribdNessuna valutazione finora
- Researchassessment3 10 20 17Documento3 pagineResearchassessment3 10 20 17api-376814514Nessuna valutazione finora
- HY GeneticsDocumento104 pagineHY Geneticsndifor bonnyNessuna valutazione finora
- 292-Article Text-1640-1-10-20190515Documento8 pagine292-Article Text-1640-1-10-20190515Liset Edreira Cutipa SallucaNessuna valutazione finora
- Dwarfism Essays Research PapersDocumento8 pagineDwarfism Essays Research Papersljkwfwgkf100% (1)
- AchondroplasiaDocumento3 pagineAchondroplasiaramziaNessuna valutazione finora
- 1223 FullDocumento9 pagine1223 FullElla AnggRainiNessuna valutazione finora
- Research Paper On Down Syndrome PDFDocumento6 pagineResearch Paper On Down Syndrome PDFfzkk43h9100% (1)
- Pediatric Neurologic Physical TherapyDocumento38 paginePediatric Neurologic Physical TherapyfagpatelNessuna valutazione finora
- The Beginners Guide To SEODocumento54 pagineThe Beginners Guide To SEOIkechukwu OkeyNessuna valutazione finora
- Health It StatisticsDocumento53 pagineHealth It Statisticssavvy_as_98-1Nessuna valutazione finora
- BMJ PicoDocumento6 pagineBMJ Picosavvy_as_98-1Nessuna valutazione finora
- Assessing Nasal Air FlowDocumento9 pagineAssessing Nasal Air Flowsavvy_as_98-1Nessuna valutazione finora
- Problem Solving ModelDocumento6 pagineProblem Solving ModelHamet Huallpa Paz100% (1)
- Quality Measures For Care of Patients With InsomniaDocumento6 pagineQuality Measures For Care of Patients With Insomniasavvy_as_98-1Nessuna valutazione finora
- Governance MetricsDocumento12 pagineGovernance Metricssavvy_as_98-1Nessuna valutazione finora
- Skinny TzatzikiDocumento28 pagineSkinny Tzatzikisavvy_as_98-1Nessuna valutazione finora
- Propriospinal MyoclonusDocumento9 paginePropriospinal Myoclonussavvy_as_98-1Nessuna valutazione finora
- Future of CMIO Role in Value-Based HealthcareDocumento5 pagineFuture of CMIO Role in Value-Based Healthcaresavvy_as_98-1Nessuna valutazione finora
- Clinical Informaticist VacancyDocumento1 paginaClinical Informaticist Vacancysavvy_as_98-1Nessuna valutazione finora
- Data MiningDocumento50 pagineData Miningsavvy_as_98-1Nessuna valutazione finora
- Sleep TelemedicineDocumento11 pagineSleep Telemedicinesavvy_as_98-1Nessuna valutazione finora
- Analysis of German Credit DataDocumento24 pagineAnalysis of German Credit Datasavvy_as_98-1100% (1)
- Challenges of Precision Medicine in OSADocumento14 pagineChallenges of Precision Medicine in OSAsavvy_as_98-1Nessuna valutazione finora
- Weight Gain and CpapDocumento3 pagineWeight Gain and Cpapsavvy_as_98-1Nessuna valutazione finora
- Chronopharmacology of Anti Convulsive TherapyDocumento15 pagineChronopharmacology of Anti Convulsive Therapysavvy_as_98-1Nessuna valutazione finora
- Future of CMIO Role in Value-Based HealthcareDocumento5 pagineFuture of CMIO Role in Value-Based Healthcaresavvy_as_98-1Nessuna valutazione finora
- What Is Data Mining in HealthcareDocumento13 pagineWhat Is Data Mining in Healthcaresavvy_as_98-1Nessuna valutazione finora
- Mobile Devices and InsomniaDocumento6 pagineMobile Devices and Insomniasavvy_as_98-1Nessuna valutazione finora
- Psychology of LeadershipDocumento16 paginePsychology of Leadershipsavvy_as_98-1Nessuna valutazione finora
- CPOE Clinical Workflow Analysis PDFDocumento59 pagineCPOE Clinical Workflow Analysis PDFsavvy_as_98-1Nessuna valutazione finora
- Bicep Curl To Shoulder PressDocumento5 pagineBicep Curl To Shoulder Presssavvy_as_98-1Nessuna valutazione finora
- SDB and Stroke Therapeutic ApproachesDocumento8 pagineSDB and Stroke Therapeutic Approachessavvy_as_98-1Nessuna valutazione finora
- Neuroimaging Insights Into InsomniaDocumento7 pagineNeuroimaging Insights Into Insomniasavvy_as_98-1Nessuna valutazione finora
- Data Mining AlgorithmsDocumento6 pagineData Mining Algorithmssavvy_as_98-1Nessuna valutazione finora
- Role of Nasal Surgery in OsaDocumento5 pagineRole of Nasal Surgery in Osasavvy_as_98-1Nessuna valutazione finora
- Neurobiology and Neuropathophysiology of OsaDocumento12 pagineNeurobiology and Neuropathophysiology of Osasavvy_as_98-1Nessuna valutazione finora
- Escape Room 3Documento6 pagineEscape Room 3jenniferNessuna valutazione finora
- Family Pedigree Project KennedyDocumento4 pagineFamily Pedigree Project KennedySian LouNessuna valutazione finora
- Sex Determination and Sex LinkedpptxDocumento47 pagineSex Determination and Sex LinkedpptxJanloydNessuna valutazione finora
- Pinongpong-Mendelian Genetics 2Documento8 paginePinongpong-Mendelian Genetics 2Jonald PINONGPONGNessuna valutazione finora
- Plant BreedingDocumento36 paginePlant BreedingRhene BarcelonNessuna valutazione finora
- Worksheet - Non-Mendelian TraitsDocumento4 pagineWorksheet - Non-Mendelian TraitsJude GNessuna valutazione finora
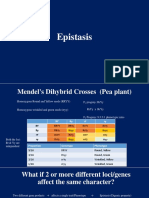
- Epistasis (Lect 16 & 17)Documento15 pagineEpistasis (Lect 16 & 17)Erum JanNessuna valutazione finora
- Sex Linked Inheritance Pedigree 2016Documento37 pagineSex Linked Inheritance Pedigree 2016Krisburt Delos SantosNessuna valutazione finora
- Student Exploration: Evolution: Mutation and SelectionDocumento7 pagineStudent Exploration: Evolution: Mutation and SelectionStephanie ValienteNessuna valutazione finora
- Lesson 1Documento15 pagineLesson 1Vim Dela Cruz EnobioNessuna valutazione finora
- Genetic SymbolsDocumento3 pagineGenetic SymbolsHoney McRueloNessuna valutazione finora
- Cambridge IGCSE: BIOLOGY 0610/43Documento24 pagineCambridge IGCSE: BIOLOGY 0610/43Ashtav ArunNessuna valutazione finora
- Gizmo Natural Selection Artificial SelectionDocumento7 pagineGizmo Natural Selection Artificial SelectionAshley ClarkNessuna valutazione finora
- Genetics PowerpointDocumento39 pagineGenetics PowerpointRizky EliandiNessuna valutazione finora
- Test Bank For Human Development A Life Span View Third EditionDocumento21 pagineTest Bank For Human Development A Life Span View Third Editionsteelerversionxs9Nessuna valutazione finora
- Classical Genetics and The Theory PDFDocumento27 pagineClassical Genetics and The Theory PDFPablo LorenzanoNessuna valutazione finora
- The Third Position Free Digital EditionDocumento401 pagineThe Third Position Free Digital EditionO.E. Nordahl100% (1)
- Problem Solving Review On Mendelian GeneticsDocumento26 pagineProblem Solving Review On Mendelian Geneticsemilla chanNessuna valutazione finora
- BIOLOGY SLK Q4 FINAL EDITED 0.2color Coded1Documento45 pagineBIOLOGY SLK Q4 FINAL EDITED 0.2color Coded1King TagabuenNessuna valutazione finora
- Mendelian Laws and Inheritance PatternsDocumento22 pagineMendelian Laws and Inheritance PatternsNau MaanNessuna valutazione finora
- Mendelian Inheritance and Extensions to Mendel's LawsDocumento27 pagineMendelian Inheritance and Extensions to Mendel's LawsWaleed AhmedNessuna valutazione finora
- ICSE BiologyDocumento10 pagineICSE BiologysubhaseduNessuna valutazione finora
- Mouse Genetics 2 SEDocumento5 pagineMouse Genetics 2 SEAmbrielle WhiteNessuna valutazione finora
- Applying Mendel's Principles: Getting StartedDocumento6 pagineApplying Mendel's Principles: Getting Startedlk vocalNessuna valutazione finora
- Essential Notes On Pathophysiology For Advanced Practice NursesDocumento88 pagineEssential Notes On Pathophysiology For Advanced Practice NursesHaneenNessuna valutazione finora
- Dihybrid Cross Practice ProblemsDocumento7 pagineDihybrid Cross Practice Problemsbrenden chapmanNessuna valutazione finora
- BIOF11 Tutorial 7Documento5 pagineBIOF11 Tutorial 7Rachna LalNessuna valutazione finora
- Lab 05 MicroevolutionDocumento24 pagineLab 05 MicroevolutionYanirRamziNessuna valutazione finora
- SPM Biology F5C5 Inheritance (Presentation)Documento65 pagineSPM Biology F5C5 Inheritance (Presentation)Lee KaiYangNessuna valutazione finora
- Class 12-Chapter 5 Principles of InheritanceDocumento5 pagineClass 12-Chapter 5 Principles of InheritanceSaransh KumarNessuna valutazione finora