Potrebbero piacerti anche
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- Telmisartan AmlodipineDocumento10 pagineTelmisartan AmlodipineDeby Tri Widia LestariNessuna valutazione finora
- Disease of Adrenal Gland: Dr. Fatimah Eliana, SPPD, KemdDocumento57 pagineDisease of Adrenal Gland: Dr. Fatimah Eliana, SPPD, KemdDeby Tri Widia LestariNessuna valutazione finora
- Syok KardiogenikDocumento31 pagineSyok KardiogenikcantikarevieraNessuna valutazione finora
- HonkDocumento11 pagineHonkYozhanNessuna valutazione finora
- Osteoporosis F DHDocumento39 pagineOsteoporosis F DH95kodok85Nessuna valutazione finora
- KadDocumento25 pagineKadraisaNessuna valutazione finora
- Japan Earthquake HighlightedDocumento3 pagineJapan Earthquake HighlightedDeby Tri Widia LestariNessuna valutazione finora
- 0704 06Documento4 pagine0704 06Deby Tri Widia LestariNessuna valutazione finora
- P Knowlesi PDFDocumento3 pagineP Knowlesi PDFNurbieber Saiianklylavrilavigne BieberNessuna valutazione finora
- Kuliah Obat Esensial Dan FormulariumDocumento12 pagineKuliah Obat Esensial Dan FormulariumNita RahmatunnisaNessuna valutazione finora
- Sexual Violence Sept 2014 152Documento6 pagineSexual Violence Sept 2014 152Deby Tri Widia LestariNessuna valutazione finora
- Prevalence of Anemia Risk Factors in Pregnant Women in Kerman, IranDocumento4 paginePrevalence of Anemia Risk Factors in Pregnant Women in Kerman, IranDeby Tri Widia LestariNessuna valutazione finora
- GPQ 20 Jun08 PDFDocumento4 pagineGPQ 20 Jun08 PDFDeby Tri Widia LestariNessuna valutazione finora
- Konsumsi Makanan Dan Kejadian Anemia Pada Siswi Salah Satu SMP Di Kota MakassarDocumento4 pagineKonsumsi Makanan Dan Kejadian Anemia Pada Siswi Salah Satu SMP Di Kota MakassarTegoeh RizkiNessuna valutazione finora
- Life Stress TestDocumento2 pagineLife Stress Test95kodok85Nessuna valutazione finora
- Headache QuestionnaireDocumento10 pagineHeadache QuestionnairePerisha VeeraNessuna valutazione finora
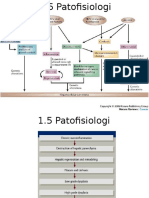
- 1.5 Patofisiologi Karsinoma HepatoselulerDocumento2 pagine1.5 Patofisiologi Karsinoma HepatoselulerDeby Tri Widia LestariNessuna valutazione finora
- Stress Dan AnxietasDocumento4 pagineStress Dan AnxietasIhsan Rasyid YuldiNessuna valutazione finora
- IndianJMedSci6611-3703196 101711Documento12 pagineIndianJMedSci6611-3703196 10171195kodok85Nessuna valutazione finora
- Prevalence of Stress Among Medical Students in Jizan University Kingdom of Saudi ArabiaDocumento7 paginePrevalence of Stress Among Medical Students in Jizan University Kingdom of Saudi ArabiaDeby Tri Widia LestariNessuna valutazione finora
- VaksinasiDocumento9 pagineVaksinasiDeby Tri Widia LestariNessuna valutazione finora
- 15Documento5 pagine15Deby Tri Widia LestariNessuna valutazione finora
- Migraine Prevalence, Alexithymia, and Post-Traumatic StressDocumento9 pagineMigraine Prevalence, Alexithymia, and Post-Traumatic StressDeby Tri Widia LestariNessuna valutazione finora
- Konsumsi Makanan Dan Kejadian Anemia Pada Siswi Salah Satu SMP Di Kota MakassarDocumento4 pagineKonsumsi Makanan Dan Kejadian Anemia Pada Siswi Salah Satu SMP Di Kota MakassarTegoeh RizkiNessuna valutazione finora
- Epidemiological Investigation of A Temporal Increase in Atonic Postpartum Haemorrhage A Population-Based Retrospective Cohort StudyDocumento10 pagineEpidemiological Investigation of A Temporal Increase in Atonic Postpartum Haemorrhage A Population-Based Retrospective Cohort StudyDeby Tri Widia LestariNessuna valutazione finora
- Exsanguinated Uterus After Massive Atonic Postpartum HaemorrhageDocumento4 pagineExsanguinated Uterus After Massive Atonic Postpartum HaemorrhageDeby Tri Widia LestariNessuna valutazione finora
- Postpartum Haemorrhage in Midwifery Care in The Netherlands Validation of Quality Indicators For Midwifery GuidelinesDocumento6 paginePostpartum Haemorrhage in Midwifery Care in The Netherlands Validation of Quality Indicators For Midwifery GuidelinesDeby Tri Widia LestariNessuna valutazione finora
- Maternal Near Miss in Rural Hospital SudanDocumento4 pagineMaternal Near Miss in Rural Hospital SudanVikas LonikarNessuna valutazione finora
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (344)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (399)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (588)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (73)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2259)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (120)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)