Potrebbero piacerti anche
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5794)
- v085p00848 PDFDocumento7 paginev085p00848 PDFmiftahul masruriNessuna valutazione finora
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- Leaflet LansiaDocumento1 paginaLeaflet Lansiamiftahul masruriNessuna valutazione finora
- HH PowerPointDocumento36 pagineHH PowerPointLailiya UchiiNessuna valutazione finora
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- Primary Iris Melanoma: Diagnostic Features and Outcome of Conservative Surgical TreatmentDocumento7 paginePrimary Iris Melanoma: Diagnostic Features and Outcome of Conservative Surgical Treatmentmiftahul masruriNessuna valutazione finora
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (895)
- Effects of Smoking Intervention and The Use of An Inhaled Anticholinergic Bronchodilator On The Rate If Decline of FEVDocumento22 pagineEffects of Smoking Intervention and The Use of An Inhaled Anticholinergic Bronchodilator On The Rate If Decline of FEVmiftahul masruriNessuna valutazione finora
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (344)
- Drug Safety AlertDocumento92 pagineDrug Safety AlertFungky AnthonyNessuna valutazione finora
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (399)
- The Tobacco Atlas (Ringkasan)Documento4 pagineThe Tobacco Atlas (Ringkasan)miftahul masruriNessuna valutazione finora
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (588)
- Suara Jantung PresentasiDocumento48 pagineSuara Jantung Presentasimiftahul masruriNessuna valutazione finora
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- The Tobacco AtlasDocumento185 pagineThe Tobacco Atlasmiftahul masruriNessuna valutazione finora
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (266)
- Drug Safety AlertDocumento92 pagineDrug Safety AlertFungky AnthonyNessuna valutazione finora
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- Effects of Smoking Intervention and The Use of An Inhaled Anticholinergic Bronchodilator On The Rate If Decline of FEVDocumento22 pagineEffects of Smoking Intervention and The Use of An Inhaled Anticholinergic Bronchodilator On The Rate If Decline of FEVmiftahul masruriNessuna valutazione finora
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- American Thoracic Society Cigarette Smfvfvoking and Health 1Documento5 pagineAmerican Thoracic Society Cigarette Smfvfvoking and Health 1miftahul masruriNessuna valutazione finora
- Effects of Smoking Intervention and The Use of An Inhaled Anticholinergic Bronchodilator On The Rate If Decline of FEVDocumento22 pagineEffects of Smoking Intervention and The Use of An Inhaled Anticholinergic Bronchodilator On The Rate If Decline of FEVmiftahul masruriNessuna valutazione finora
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (73)
- The Tobacco Atlas (Ringkasan)Documento4 pagineThe Tobacco Atlas (Ringkasan)miftahul masruriNessuna valutazione finora
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- American Thoracic Society Cigarette Smoking and Health 2Documento4 pagineAmerican Thoracic Society Cigarette Smoking and Health 2miftahul masruriNessuna valutazione finora
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- American Thoracic Society Cigarette Smoking and Health 2Documento5 pagineAmerican Thoracic Society Cigarette Smoking and Health 2miftahul masruriNessuna valutazione finora
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2259)
- Interventional BronchosDocumento323 pagineInterventional BronchosFranspol100% (1)
- Cellular AberrationDocumento71 pagineCellular AberrationKris TejereroNessuna valutazione finora
- PresentasiDocumento30 paginePresentasiagusNessuna valutazione finora
- Cancer Progress and Priorities Lung CancerDocumento18 pagineCancer Progress and Priorities Lung CancerdavidNessuna valutazione finora
- Effect of Intrathecal Hal.23Documento72 pagineEffect of Intrathecal Hal.23YayaNessuna valutazione finora
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- Production and Sales of Tobacco Must Be Made IllegalDocumento6 pagineProduction and Sales of Tobacco Must Be Made IllegalDishari PoddarNessuna valutazione finora
- Pathophysiology Patient's DataDocumento3 paginePathophysiology Patient's DataKristian Karl Bautista Kiw-isNessuna valutazione finora
- SBRT PDFDocumento14 pagineSBRT PDFrubenNessuna valutazione finora
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- Major R Cance Er Miles Stones: Overvie EwDocumento14 pagineMajor R Cance Er Miles Stones: Overvie Ewtkobosz4877Nessuna valutazione finora
- Ejsr 72 3 04Documento9 pagineEjsr 72 3 04Khalifa BakkarNessuna valutazione finora
- Companion Diagnostics or Theranostics Products in The MarketDocumento3 pagineCompanion Diagnostics or Theranostics Products in The MarkettonnymjohnsonNessuna valutazione finora
- The Positive and Negative Effects of Marijuana To HumanDocumento23 pagineThe Positive and Negative Effects of Marijuana To HumanMayeiaElenorNessuna valutazione finora
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (120)
- Case Presentation October 2015Documento30 pagineCase Presentation October 2015api-312376917100% (1)
- 211004961.04 - Pasimun - RSUP Dr. M. DjamilDocumento1 pagina211004961.04 - Pasimun - RSUP Dr. M. DjamilLycka AkaishaNessuna valutazione finora
- Immunotherapy For Lung CancerDocumento3 pagineImmunotherapy For Lung CancerPongwirat ChantasoontornNessuna valutazione finora
- HOW LONG HAVE I GOT LEFT, Paul KalanithiDocumento5 pagineHOW LONG HAVE I GOT LEFT, Paul KalanithiNeelansh ButeNessuna valutazione finora
- 382 FullDocumento23 pagine382 FullRahma WirdaNessuna valutazione finora
- Case Study I - Cigarette Smoking in Lung CancerDocumento12 pagineCase Study I - Cigarette Smoking in Lung CancerDavid AcuñaNessuna valutazione finora
- Biomedical Research Associate Scientist in Houston TX Resume Sandhya DasDocumento6 pagineBiomedical Research Associate Scientist in Houston TX Resume Sandhya DasSandhyaDas2100% (1)
- Vocal Cord Paralysis and Its Etiologies A Prospective StudyDocumento4 pagineVocal Cord Paralysis and Its Etiologies A Prospective StudySheilla KhonadaNessuna valutazione finora
- Discharge Planning ProjectDocumento6 pagineDischarge Planning Projectapi-282958026Nessuna valutazione finora
- Bronchogenic Carcinoma: DR Ayman El-DibDocumento40 pagineBronchogenic Carcinoma: DR Ayman El-DibMuhdZaeedNessuna valutazione finora
- Liver Prime PPPDocumento17 pagineLiver Prime PPPParimal P. DubeyNessuna valutazione finora
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- Perception of Cancer in Patients Diagnosedwith The Most Common Gastrointestinalcancers PDFDocumento12 paginePerception of Cancer in Patients Diagnosedwith The Most Common Gastrointestinalcancers PDFdwiyantoroNessuna valutazione finora
- Eating For Energy NEWDocumento272 pagineEating For Energy NEWCARLOSWAR101100% (4)
- Lung Cancer (Nursing Care)Documento5 pagineLung Cancer (Nursing Care)heiyuNessuna valutazione finora
- Pulmonary Sclerosing Pneumocytoma - A Comprehensive Exploration of Clinical, Radiological, and Surgical DimensionsDocumento6 paginePulmonary Sclerosing Pneumocytoma - A Comprehensive Exploration of Clinical, Radiological, and Surgical DimensionsInternational Journal of Innovative Science and Research TechnologyNessuna valutazione finora
- Radiation-Induced Lung Injury - UpToDateDocumento38 pagineRadiation-Induced Lung Injury - UpToDateTatiana Valencia CastañoNessuna valutazione finora
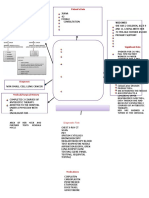
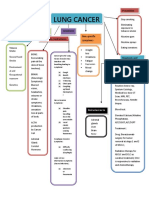
- Concept Map LungDocumento1 paginaConcept Map LungThea Eya FayeNessuna valutazione finora
- Health Effects of Secondhand SmokeDocumento4 pagineHealth Effects of Secondhand SmokeCris Tarrazona CasipleNessuna valutazione finora
- Summary: Fast Like a Girl: A Woman’s Guide to Using the Healing Power of Fasting to Burn Fat, Boost Energy, and Balance Hormones: Key Takeaways, Summary and AnalysisDa EverandSummary: Fast Like a Girl: A Woman’s Guide to Using the Healing Power of Fasting to Burn Fat, Boost Energy, and Balance Hormones: Key Takeaways, Summary and AnalysisValutazione: 3 su 5 stelle3/5 (2)