Potrebbero piacerti anche
- Empirical Prescribing Chart GlasgowDocumento1 paginaEmpirical Prescribing Chart GlasgowHariharan Narendran75% (4)
- Pediatric Acute Sepsis: Physician'S OrdersDocumento4 paginePediatric Acute Sepsis: Physician'S OrdersSughosh MitraNessuna valutazione finora
- MIS C Algorithim Version 2Documento8 pagineMIS C Algorithim Version 2Saima UmairNessuna valutazione finora
- Sickle - Cell - Guidelines TTTDocumento2 pagineSickle - Cell - Guidelines TTTAhmed BadrNessuna valutazione finora
- 2012 Aug IMG Poster 165760a SepsisDocumento1 pagina2012 Aug IMG Poster 165760a SepsisTeng Huei LeeNessuna valutazione finora
- Management of SepsisDocumento34 pagineManagement of SepsisTamim IshtiaqueNessuna valutazione finora
- UTI Treatment Algorithm - Sharp Mesa Vista 2Documento3 pagineUTI Treatment Algorithm - Sharp Mesa Vista 2Fitri 1997Nessuna valutazione finora
- Antibiotic Guidelines For BONE AND JOINT INFECTIONSDocumento3 pagineAntibiotic Guidelines For BONE AND JOINT INFECTIONSKhurram NadeemNessuna valutazione finora
- BCCA AB in Febrile Neutropenia GuidelinesDocumento2 pagineBCCA AB in Febrile Neutropenia GuidelinesAlvy SyukrieNessuna valutazione finora
- IMG EmpAposterDocumento1 paginaIMG EmpAposterChiu LeoNessuna valutazione finora
- SOP Neutropenic PatientDocumento7 pagineSOP Neutropenic Patientdrsp2001Nessuna valutazione finora
- SOP Neutropenic PatientDocumento7 pagineSOP Neutropenic Patientdrsp2001Nessuna valutazione finora
- Skin and Soft Tissue Infections - HandoutDocumento6 pagineSkin and Soft Tissue Infections - Handoutapi-641524095Nessuna valutazione finora
- HarrisonsDocumento117 pagineHarrisonsEm TimbolNessuna valutazione finora
- 2.fahad Khaliq.... Febrile Neutro - pptx-1Documento38 pagine2.fahad Khaliq.... Febrile Neutro - pptx-1dr FAHADKHALIQSIALNessuna valutazione finora
- 2.fahad Khaliq.... Febrile Neutro - pptx-1Documento38 pagine2.fahad Khaliq.... Febrile Neutro - pptx-1dr FAHADKHALIQSIALNessuna valutazione finora
- Febrile Neutropenia Final 7-29Documento74 pagineFebrile Neutropenia Final 7-29Juliyanti FuNessuna valutazione finora
- Monkeypox Protocol - V1.0 (2047833421)Documento5 pagineMonkeypox Protocol - V1.0 (2047833421)Syed AhmedNessuna valutazione finora
- Rheumatology SBIM Part 1 High Yield FactsDocumento5 pagineRheumatology SBIM Part 1 High Yield FactsGousay AlkhazmariNessuna valutazione finora
- 17.guidelines PneumoniaDocumento3 pagine17.guidelines PneumoniaRed DevilNessuna valutazione finora
- Principles of Periodontal SurgryDocumento106 paginePrinciples of Periodontal SurgrynusreenNessuna valutazione finora
- PcolDocumento17 paginePcolThea JulianaNessuna valutazione finora
- Chapter 4d Podiatric Infectious DiseasesDocumento20 pagineChapter 4d Podiatric Infectious DiseasespodmmgfNessuna valutazione finora
- Shivani PDFDocumento3 pagineShivani PDFdeepukumarNessuna valutazione finora
- Bakteriemia, Sepsis Dan Syok Septik: DR Putra Hendra SPPD UnibaDocumento33 pagineBakteriemia, Sepsis Dan Syok Septik: DR Putra Hendra SPPD UnibaTondy HarahapNessuna valutazione finora
- Department of Surgery G.R. Medical College, Gwalior: Septic Shock and Its ManagementDocumento31 pagineDepartment of Surgery G.R. Medical College, Gwalior: Septic Shock and Its ManagementNitin AggarwalNessuna valutazione finora
- Allergy and Immunology 2023 FINALDocumento18 pagineAllergy and Immunology 2023 FINALBelinda ELISHANessuna valutazione finora
- UTI Treatment Guidelines PDFDocumento5 pagineUTI Treatment Guidelines PDFMuhammad IhsanuddinNessuna valutazione finora
- Drug Study (Pe)Documento15 pagineDrug Study (Pe)Jobelle AcenaNessuna valutazione finora
- 07 - 10 - 21 Treatment of Covid 19 InfectionDocumento26 pagine07 - 10 - 21 Treatment of Covid 19 InfectionStonefalconNessuna valutazione finora
- Orthopaedic Infection in Adults UHL GuidelineDocumento10 pagineOrthopaedic Infection in Adults UHL GuidelineFadlu ManafNessuna valutazione finora
- CVS Blood PDFDocumento103 pagineCVS Blood PDF182 ROHIL HNessuna valutazione finora
- Pneumonia Management ProtocolDocumento2 paginePneumonia Management Protocolsky nuts100% (1)
- Arthritis, Infectious, BacterialDocumento6 pagineArthritis, Infectious, BacterialHarry IsraNessuna valutazione finora
- COVID-19 Disease SeverityDocumento7 pagineCOVID-19 Disease SeverityParishan SaeedNessuna valutazione finora
- Step 3 NotesDocumento4 pagineStep 3 Notesjhk0428Nessuna valutazione finora
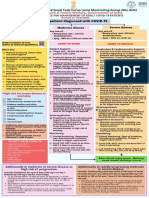
- Adult Patient Diagnosed With COVID-19: Ministry of Health & Family Welfare, Government of IndiaDocumento1 paginaAdult Patient Diagnosed With COVID-19: Ministry of Health & Family Welfare, Government of Indiapramodbankhele3845Nessuna valutazione finora
- Sarpa All BasicsDocumento11 pagineSarpa All BasicsRavichandra MentheNessuna valutazione finora
- Systemic Lupus Erythematosus Lecture Salah Abdel BakyDocumento8 pagineSystemic Lupus Erythematosus Lecture Salah Abdel Bakyahmed gabrNessuna valutazione finora
- Dr. Dian Kusumaningrum - PRESENTASI JCCA-ANTIBIOTIC DOSING IN CRITICALLY ILLDocumento31 pagineDr. Dian Kusumaningrum - PRESENTASI JCCA-ANTIBIOTIC DOSING IN CRITICALLY ILLRestu TriwulandaniNessuna valutazione finora
- DR Deshinta - KIPI Dan Penanganan Syok AnafilaksisDocumento45 pagineDR Deshinta - KIPI Dan Penanganan Syok AnafilaksisTRI WIDJAJANessuna valutazione finora
- Infeksi Pada Pasien KankerDocumento18 pagineInfeksi Pada Pasien KankerSuci Fitriani SammuliaNessuna valutazione finora
- Scorpion Envenomation Treatment & Management Prehospital Care, Emergency Department Care, Medical CareDocumento12 pagineScorpion Envenomation Treatment & Management Prehospital Care, Emergency Department Care, Medical Carejoaoalmeida_1955Nessuna valutazione finora
- Rheumatic FeverDocumento39 pagineRheumatic FeverDharaneedhar AdepuNessuna valutazione finora
- Prophylaxis Action: Tetanus: Injection: 5 To 10 LF Units ofDocumento10 pagineProphylaxis Action: Tetanus: Injection: 5 To 10 LF Units ofElle RosalesNessuna valutazione finora
- Autoimmune DiseaseDocumento31 pagineAutoimmune DiseaseKHAIRUL REDZUANNessuna valutazione finora
- Malaria and LeptospirosisDocumento18 pagineMalaria and LeptospirosisRasYa DINessuna valutazione finora
- AntivenomDocumento1 paginaAntivenomAbu RaihanNessuna valutazione finora
- Dental MedicineDocumento59 pagineDental Medicinechh56k6tndNessuna valutazione finora
- Toronto IMR - Toronto Internal Medicine Review 2024 (2024, Toronto Internal Medicine Review) - Libgen - LiDocumento2.188 pagineToronto IMR - Toronto Internal Medicine Review 2024 (2024, Toronto Internal Medicine Review) - Libgen - LiHenrique Augusto LinoNessuna valutazione finora
- Management of Septic ShockDocumento33 pagineManagement of Septic ShockswatisinghnigeriaNessuna valutazione finora
- Ny Diabetic Foot Infection Antibiotic Treatment Guidelines 2020Documento1 paginaNy Diabetic Foot Infection Antibiotic Treatment Guidelines 2020Aliyu labboNessuna valutazione finora
- Notes On Genitourinary Tract InfectionsDocumento9 pagineNotes On Genitourinary Tract InfectionsSaleh Mohammad ShoaibNessuna valutazione finora
- Management of Dengue FeverDocumento31 pagineManagement of Dengue FeverDaniel RajNessuna valutazione finora
- Pharmaco Logy Imm Une Syste M Drugs: Julia Leonor Huaringa Lagomarsino, RN February 13, 2009Documento12 paginePharmaco Logy Imm Une Syste M Drugs: Julia Leonor Huaringa Lagomarsino, RN February 13, 2009julialeoNessuna valutazione finora
- CSF Findings in Community-Acquired Acute Bacterial Meningitis, MGHDocumento34 pagineCSF Findings in Community-Acquired Acute Bacterial Meningitis, MGHMhelshy VillanuevaNessuna valutazione finora
- Infective EndocarditisDocumento57 pagineInfective EndocarditisRika FitriaNessuna valutazione finora
- Empirical First Line AntibioticsDocumento1 paginaEmpirical First Line Antibioticsdiati zahrainiNessuna valutazione finora
- COVID-19 Ag Test Kit: (For Medical Professional Use Only)Documento2 pagineCOVID-19 Ag Test Kit: (For Medical Professional Use Only)threwawayNessuna valutazione finora
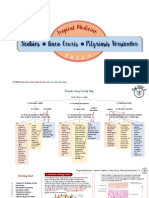
- Scabies Tinea Cruris Pityriasis Versicolor: Semangat!Documento11 pagineScabies Tinea Cruris Pityriasis Versicolor: Semangat!Fitriah Nur SyamiatiNessuna valutazione finora
- 0 - Hospital Design 2020 PDFDocumento3 pagine0 - Hospital Design 2020 PDFPriya DharshiniNessuna valutazione finora
- Case Presentation ScabiesDocumento26 pagineCase Presentation Scabieshardi auliaNessuna valutazione finora
- Henoch Schonlein Purpura GuidelineDocumento12 pagineHenoch Schonlein Purpura GuidelinewenyinriantoNessuna valutazione finora
- Journal Reading: Stase Ilmu THT RS Umum Daerah Sayang Cianjur Universitas Muhammadiyah Jakarta 2019Documento15 pagineJournal Reading: Stase Ilmu THT RS Umum Daerah Sayang Cianjur Universitas Muhammadiyah Jakarta 2019dwi purwantiNessuna valutazione finora
- Lecture 16 Clinical Aspect NeuroDocumento25 pagineLecture 16 Clinical Aspect NeuroByron MacalintalNessuna valutazione finora
- TN MRB Auxiliary Nurse Midwife Exam SyllabusDocumento4 pagineTN MRB Auxiliary Nurse Midwife Exam SyllabusmathanbhuNessuna valutazione finora
- Allergies or Food Intolerances.: Therapeutic DietDocumento3 pagineAllergies or Food Intolerances.: Therapeutic DietBryan Mae H. DegorioNessuna valutazione finora
- Pharmacology of Phenadoxone dN-Morpholino 4:4 Diphenyl: HydrochlorideDocumento17 paginePharmacology of Phenadoxone dN-Morpholino 4:4 Diphenyl: Hydrochlorideisaev201Nessuna valutazione finora
- HSV1 HSV2 R-Gene & VZV R-GeneDocumento2 pagineHSV1 HSV2 R-Gene & VZV R-GeneSachinNessuna valutazione finora
- Icd-10 Oktober 2021Documento9 pagineIcd-10 Oktober 2021Nia KurniawatiNessuna valutazione finora
- Reckettsia and ChlamediaDocumento37 pagineReckettsia and ChlamediaMuqtadir “The Ruler” KuchikiNessuna valutazione finora
- Management of Anembryonic Pregnancy Loss: An Observational StudyDocumento6 pagineManagement of Anembryonic Pregnancy Loss: An Observational StudyAnonymous ORleRrNessuna valutazione finora
- Eye Docs GlaucomaDocumento147 pagineEye Docs GlaucomaMuneeb ShahzadNessuna valutazione finora
- Resume Tatiana HajouDocumento1 paginaResume Tatiana Hajouapi-338525355Nessuna valutazione finora
- InTech-Yamamoto New Scalp Acupuncture Ynsa Development Principles Safety Effectiveness and Clinical ApplicationsDocumento17 pagineInTech-Yamamoto New Scalp Acupuncture Ynsa Development Principles Safety Effectiveness and Clinical Applicationsdasamoro100% (3)
- Mastectomy: Presenter: DR Janardhan T Post GraduateDocumento49 pagineMastectomy: Presenter: DR Janardhan T Post GraduateASHUTOSH KUMARNessuna valutazione finora
- DVH LimitsDocumento1 paginaDVH LimitsDioni SandovalNessuna valutazione finora
- Art Therapy What Is Art Therapy?Documento2 pagineArt Therapy What Is Art Therapy?rohit singhNessuna valutazione finora
- A Case of Paediatric CholelithiasisDocumento4 pagineA Case of Paediatric CholelithiasisHomoeopathic PulseNessuna valutazione finora
- List of Top Level Categories: CHAPTER 01 Certain Infectious or Parasitic DiseasesDocumento148 pagineList of Top Level Categories: CHAPTER 01 Certain Infectious or Parasitic Diseasesျပည္ စိုးNessuna valutazione finora
- First AID For The USMLE Public HealthDocumento20 pagineFirst AID For The USMLE Public HealthLilit M-yanNessuna valutazione finora
- Craniocerebral TraumaDocumento64 pagineCraniocerebral TraumaBentoys StreetNessuna valutazione finora
- Twin Block Case ReportDocumento5 pagineTwin Block Case ReportwjeelaniNessuna valutazione finora
- M4 - Didactic - NCM 118Documento4 pagineM4 - Didactic - NCM 118KARL FESARITNessuna valutazione finora
- Diagnosis of Midface Fractures With CT: What The Surgeon Needs To KnowDocumento24 pagineDiagnosis of Midface Fractures With CT: What The Surgeon Needs To KnowMohammad AdhityaNessuna valutazione finora
- Faculty List2019Documento6 pagineFaculty List2019suyashsahu2505Nessuna valutazione finora
- CDC 26714 DS1Documento383 pagineCDC 26714 DS1Joyce AngobungNessuna valutazione finora
- Bac AmpicillinDocumento2 pagineBac AmpicillinAnkush BiswasNessuna valutazione finora